Prajjwol D. Bhatta, MD1, Mahesh Nepal, MD1, Asim Mushtaq, MD2, Tariq Alamin, MBBS1, Joel L. Shapiro, MD1 1Rochester General Hospital, Rochester, NY; 2Rochester Regional Health, Rochester, NY Introduction: Trastuzumab-emtansine (T-DM1), is an antibody-drug conjugate composed of trastuzumab, a thioether linker (SMCC), and emtansine (DM1). Upon binding to HER2, T-DM1 is internalized and undergoes proteolytic digestion, releasing the cytotoxic microtubule inhibitor within the target cells. Common adverse reactions to T-DM1 are nausea, thrombocytopenia, increased liver aminotransferases. Herein we report a case of non-cirrhotic portal hypertension caused by nodular regenerative hyperplasia (NRH) following T-DM1 therapy.
Case Description/
Methods: A 74-year-old woman with HER2-positive metastatic breast cancer, on trastuzumab emtansine since 12/2018, presented with progressive lower extremity edema, abdominal distension, and dyspnea. Her last dose of T-DM1 was two months back. Lab work up revealed thrombocytopenia, hyperbilirubinemia, mild transaminitis.US doppler showed ascites, lobulated liver contour, and patent hepatic and portal veins. Patient underwent trans jugular liver biopsy which revealed NRH with patchy sinusoidal fibrosis, without bridging fibrosis or cirrhosis. Her HVPG was 14mmhg, confirming portal hypertension. Her hepatitis panel was negative, autoimmune serologies, ferritin, ceruloplasmin all were within normal range. Following discontinuation of trastuzumab, liver tests and platelets normalized. Discussion: Drug-induced NRH is rare and typically occurs after months or years of treatment. It is a diffuse transformation of normal hepatic parenchyma into small and regenerative nodules, with little to no fibrosis. The likely mechanism is heterogenous hepatic perfusion. The prevalence of NRH is uncertain. There is often a latent phase of asymptomatic liver damage with a mild elevation in transaminases. NRH is diagnosed later when features of portal hypertension such as variceal bleeding, ascites, or splenomegaly appear. This case highlights the need for high index of clinical suspicion when a patient on T-DM1 presents with elevated transaminase level and hyperbilirubinemia. Therefore, such patients should be monitored closely with regular liver function tests, platelet counts, and periodic imaging.
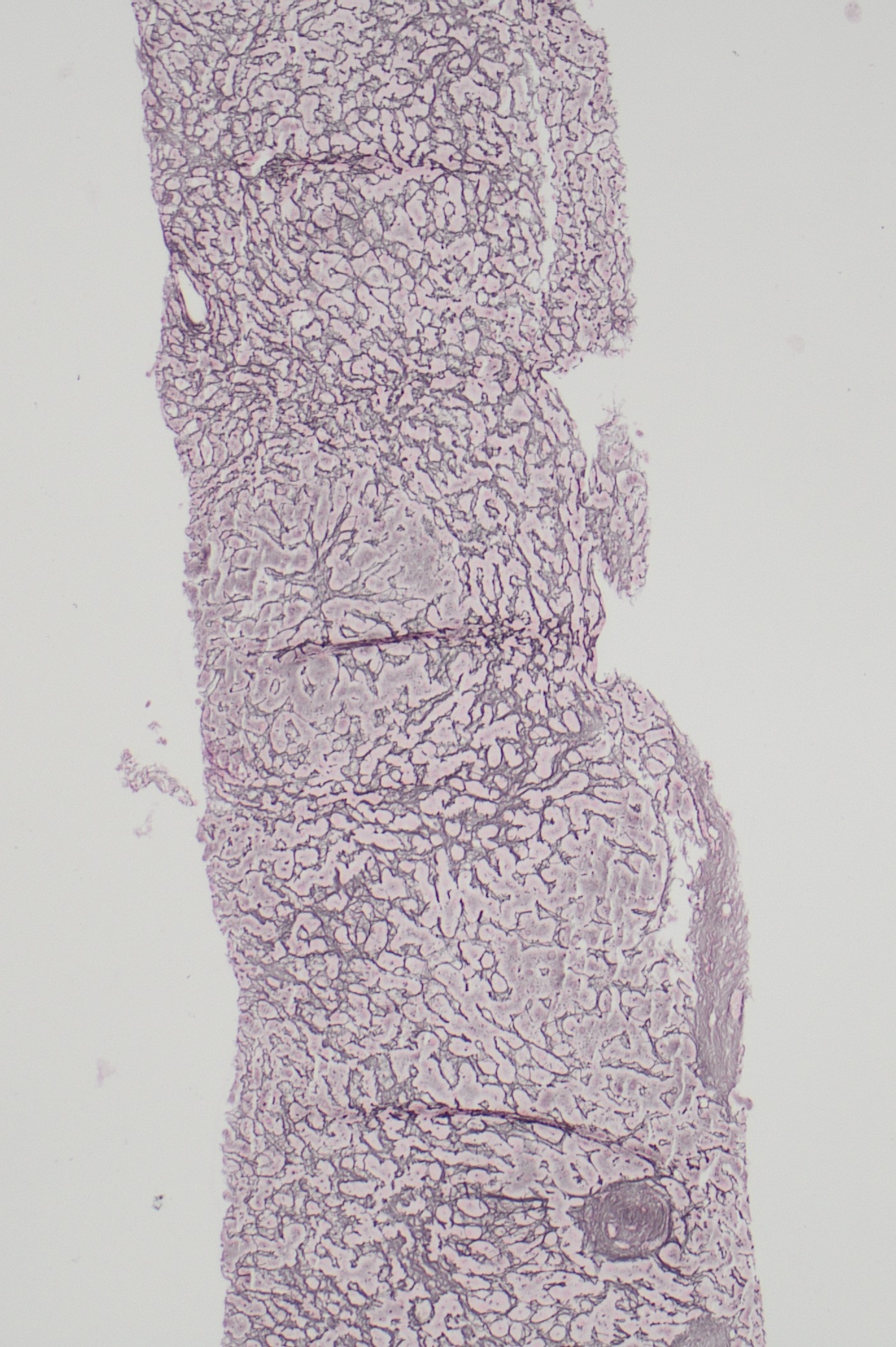
Figure: Reticulin stain showing alternate areas of hyperplastic hepatocytes adjacent to atrophic hepatocytes in nodular pattern
Disclosures: Prajjwol Bhatta indicated no relevant financial relationships. Mahesh Nepal indicated no relevant financial relationships. Asim Mushtaq indicated no relevant financial relationships. Tariq Alamin indicated no relevant financial relationships. Joel Shapiro indicated no relevant financial relationships.
Prajjwol D. Bhatta, MD1, Mahesh Nepal, MD1, Asim Mushtaq, MD2, Tariq Alamin, MBBS1, Joel L. Shapiro, MD1. P6157 - A Case of Non-Cirrhotic Portal Hypertension Secondary to Transtuzumab-Emtansine (T-DM1)-Induced Nodular Regenerative Hyperplasia (NRH), ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.