P6290 - This Too Shall Not Pass: A Multi-Disciplinary Approach to Management of Bouveret Syndrome and Proximal Duodenal Obstruction When Endoscopic Management Fails
Jared Fehlman, MD, Achraf Mansour, MD, Aram Seo, MD, Richard Nickowitz, MD Huntington Hospital, Pasadena, CA Introduction: Bouveret Syndrome is a rare complication of gallstone ileus. Caused by the impaction of a large stone in the pyloric channel/proximal duodenum and making up less than 3% of gallstone ileus cases, it is important to review this unique cause of mechanical obstruction, especially as symptoms can be vague and a delay in diagnosis can be fatal.
Case Description/
Methods: Our patient is an 81-year-old female with a history of heart failure with preserved ejection fraction, right lower extremity amputation secondary to fibrosarcoma, pre-diabetes, and perforated appendicitis a year prior, who presented with abdominal pain for 1 month. She described the pain as aching and intermittent, and additionally developed nausea, poor appetite, and frequent belching. On exam, the abdomen was soft, non-tender, with hypoactive bowel sounds, and a nasogastric tube was placed. Initial labs showed mild leukocytosis of 11.4, hemoglobin within normal limits, and normal electrolytes. In addition, there was some mild transaminitis. She did not endorse any vomiting, melena, hematochezia, or hematemesis. She had never had a colonoscopy or esophagogastroduodenoscopy (EGD). Patient had a CT abdomen pelvis with contrast, which revealed biliary duodenal fistula with multiple large gallstones within the duodenum, one of which (2.6 cm) was impacted at the duodenum and possibly causing at least a partial obstruction. The patient underwent EGD on day 2 of hospitalization with no stone identified. Patient’s obstructive symptoms began to worsen, and re-imaging with CT demonstrated a previously identified stone in the jejunum with a new 4.0 cm stone within the proximal duodenum. She underwent an exploratory laparotomy with small bowel enterotomy and removal of gallstones. The surgery was well tolerated, and she was able to start her diet and was discharged a few days after the procedure. Discussion: Our patient depicts a prototypical patient of those at risk for Bouveret Syndrome, particularly females of advanced age. This case provides a guide for which steps to take in management when EGD intervention is unsuccessful. The teaching components of this case include the early involvement of hepatobiliary surgery, the prompt diagnosis and re-imaging of the bowel to identify gallstones, and the open communication between members of the gastrointestinal and surgical team. All these factors contributed to the quick management of this patient’s obstruction, and her overall success.
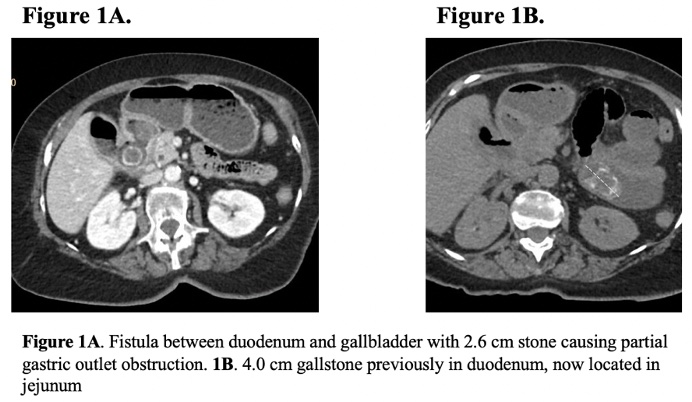
Figure: Figure 1A. Fistula between duodenum and gallbladder with 2.6 cm stone causing partial gastric outlet obstruction. 1B. 4.0 cm gallstone previously in duodenum, now located in jejunum.
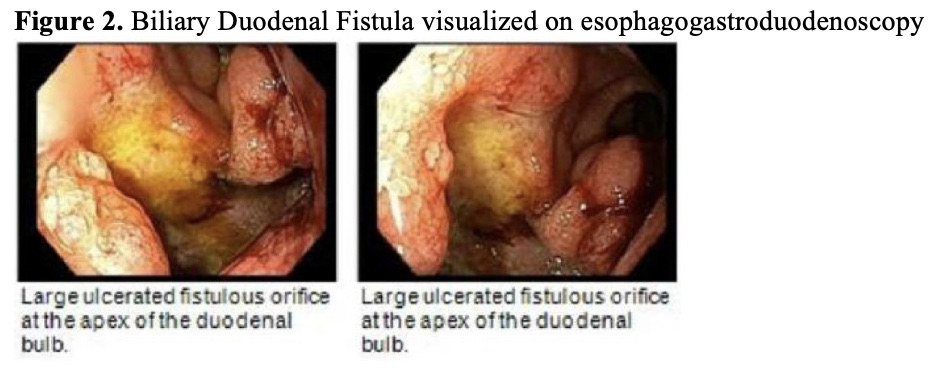
Figure: Figure 2. Biliary duodenal fistula visualized on esophagogastroduodenoscopy.
Disclosures: Jared Fehlman indicated no relevant financial relationships. Achraf Mansour indicated no relevant financial relationships. Aram Seo indicated no relevant financial relationships. Richard Nickowitz indicated no relevant financial relationships.
Jared Fehlman, MD, Achraf Mansour, MD, Aram Seo, MD, Richard Nickowitz, MD. P6290 - This Too Shall Not Pass: A Multi-Disciplinary Approach to Management of Bouveret Syndrome and Proximal Duodenal Obstruction When Endoscopic Management Fails, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")