Ivana Rubenstein, DO, Oadie Al Saleh, MD, Lloyd Bijuli-Singh, MD, Vipin Gupta, MD Broward Health Medical Center, Fort Lauderdale, FL Introduction: Superior mesenteric artery (SMA) syndrome is a rare cause of small bowel obstruction due to compression of the third portion of the duodenum between the abdominal aorta and the SMA, often secondary to mesenteric fat pad loss. Although affecting only 0.1–0.3% of the population, suspicion should remain high in patients with obstruction symptoms and recent weight loss, often due to malignancy, malabsorption, trauma, burns, HIV, or other chronic illnesses. Diagnosis is clinical and radiologic, with treatment initially focused on nutritional support. Surgical intervention is considered if conservative therapy fails.
Case Description/
Methods: A 59-year-old male with HIV and Hepatitis C presented with two weeks of nausea, vomiting, and no bowel movements for a week. He reported a 30-pound weight loss over three months and had three prior hospitalizations for similar symptoms. His social history included a 40 pack-year smoking history. Physical exam showed a distended, non-tender abdomen. Imaging revealed gastric distension. An upper GI study and small bowel series confirmed SMA syndrome, supported by MRA findings of an aortomesenteric angle < 20°.
Initial management included IV fluids and electrolyte repletion. Nutritional support with oral shakes and postural techniques was attempted but unsuccessful. The patient declined jejunostomy tube placement. With continued symptoms and failure to gain weight, he required TPN. Surgical consultation recommended gastrojejunostomy, which the patient tolerated well. Postoperatively, he advanced to a bariatric diet with normalized bowel movements. Discussion: Timely recognition of SMA syndrome is essential to prevent a cycle of obstruction and weight loss. Electrolyte derangements such as hypochloremic, hypokalemic metabolic alkalosis are common due to vomiting. Conservative therapy—including gastric decompression, postural changes, and nutritional rehabilitation—is first-line and aims to restore the mesenteric fat pad. In this case, persistent symptoms and failed enteral strategies necessitated surgical intervention. More studies are needed to define predictive markers for conservative therapy failure and to optimize nutritional interventions for SMA syndrome.
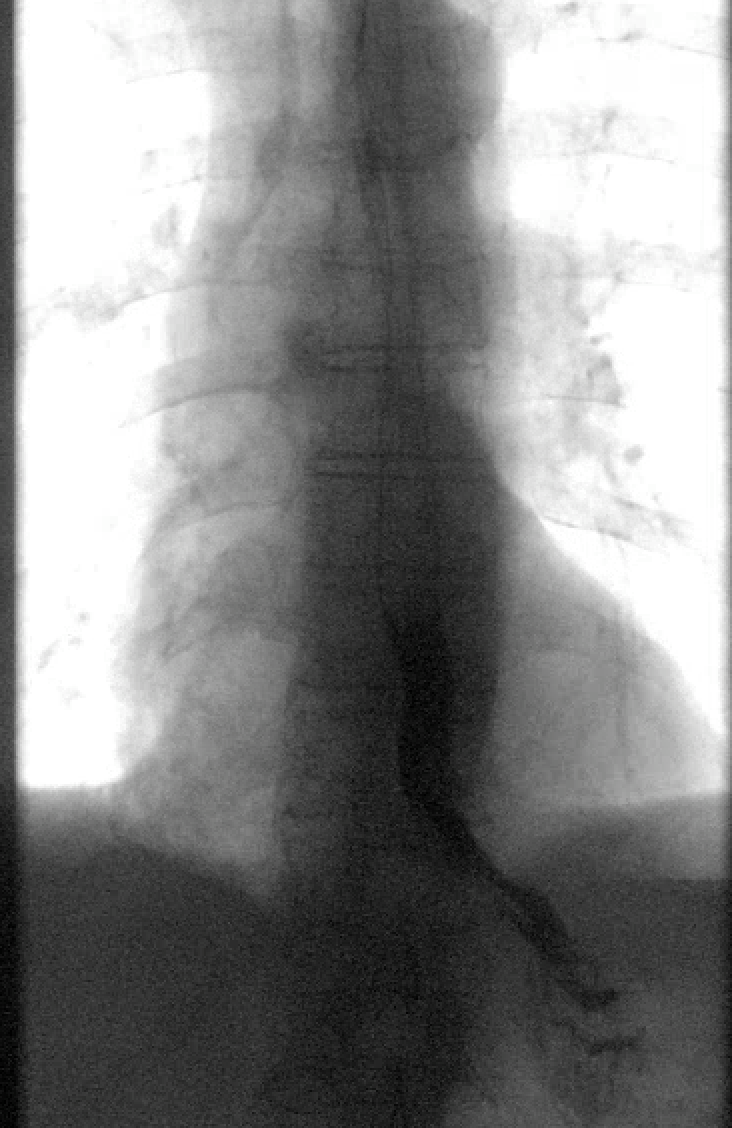
Figure: Figure 1: Snapshot of an upper GI study with small bowel series revealing SMA syndrome.
Figure: Figure 2: MRA of the abdomen showing an aortomesenteric angle of < 20 degrees.
Disclosures: Ivana Rubenstein indicated no relevant financial relationships. Oadie Al Saleh indicated no relevant financial relationships. Lloyd Bijuli-Singh indicated no relevant financial relationships. Vipin Gupta indicated no relevant financial relationships.
Ivana Rubenstein, DO, Oadie Al Saleh, MD, Lloyd Bijuli-Singh, MD, Vipin Gupta, MD. P6273 - Breaking the Cycle: A Case of Refractory SMA Syndrome Requiring Surgical Bypass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")