Nichole C. Henkes, MD, Chasen Cottle, MD, Jessica Petrov, MD, MSc, Philip Okafor, MD, MPH, FACG Mayo Clinic, Jacksonville, FL Introduction: Duodenal injury is an uncommon finding in abdominal trauma and a majority of cases occurring in pediatrics. In adults, duodenal injury is most often caused by penetrating trauma, such as stab or gunshot wounds. Due to its proximity to other organs, isolated duodenal hematomas (IDH) are rare. IDH often has a delayed, vague presentation making diagnosis a challenge. We present a rare case of gastric outlet obstruction from IDH secondary to blunt abdominal trauma.
Case Description/
Methods: A 58-year-old male presented to the emergency department for abdominal pain and vomiting. The patient reported falling down the stairs 1-2 weeks prior, landing on his back. Afterwards, he experienced abdominal pain and malaise. His wife had viral gastroenteritis at the time, and he believed he had the same affliction. The intermittent abdominal pain acutely worsened two days prior to presentation.
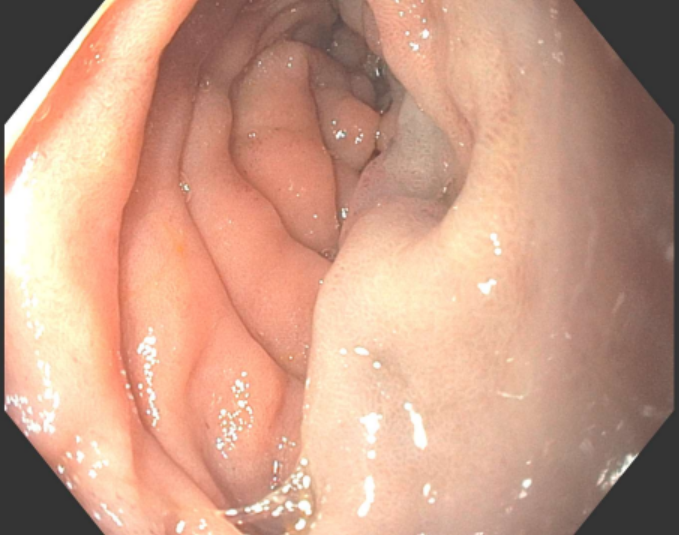
Computed tomography (CT) angiogram revealed a subacute IDH of the anterior duodenal wall with a retroperitoneal hematoma extending inferiorly from the duodenum (Figure 1). Magnetic resonance did not show any mass. Esophagogastroduodenoscopy revealed extrinsic deformity of the second/third portion of the duodenum resulting in 30-40% luminal narrowing with a bluish submucosal hue consistent with hematoma (Figure 2). No mass, bleeding or connective tissue disorder was identified, but trauma to the back seemed an implausible cause of IDH. Upon further discussion, the patient shared that he was carrying his 80-lb dog when he fell down the stairs, which landed on his abdomen.
As the patient was stable and the hematoma subacute, surgical intervention was not recommended. The patient was treated conservatively with parenteral nutrition until the obstruction resolved. Discussion: IDH is a rare finding that often presents days to weeks after injury with vague abdominal symptoms. The patient had presented to several clinics for intermittent abdominal pain, nausea and vomiting. It was not until he developed persistent vomiting and pain that the IDH was identified on CT. Our case highlights the challenges of early diagnosis, as clinicians and patients may not suspect remote abdominal trauma as the underlying cause. We also share this case to emphasize the importance of history-taking in this era of new studies and imaging modalities. Contrary to our patient, operative management of IDH due to blunt trauma is typically reserved for patients who have peritonitis, become unstable, or have complete obstruction for a prolonged period.
Figure: Figure 1. Retroperitoneal hematoma extending inferiorly from duodenum, measuring up to 11.7 x 10.1 x 8.4 cm. Another duodenal hematoma extending from the second portion of the duodenum measuring up to 8.6 x 6.2 x 8.0 cm.
Figure: Figure 2. Esophagogastroduodenoscopy (EGD) view of the second portion of the duodenum with extrinsic compression, resulting in 30-40% luminal narrowing. The submucosal wall with a bluish hue consistent with known hematoma.
Disclosures: Nichole Henkes indicated no relevant financial relationships. Chasen Cottle indicated no relevant financial relationships. Jessica Petrov indicated no relevant financial relationships. Philip Okafor indicated no relevant financial relationships.
Nichole C. Henkes, MD, Chasen Cottle, MD, Jessica Petrov, MD, MSc, Philip Okafor, MD, MPH, FACG. P6272 - The Hidden Impact: Gastric Outlet Obstruction Secondary to Isolated Duodenal Hematoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")