United Health Services, Wilson Medical Center Binghamton, NY
Ahmed Shehadah, MD1, Fawad Talat, MD1, AbdulSubhan Talpur, MD1, Usama Sakhawat, MD2, Alshaima Yousef, MD3, Khandokar Talib, MD4, Godson Senyondo, MD1, Chibuike Enwereuzo, MD1, Toseef Javaid, MD2, Amanke Oranu, MD1 1United Health Services, Wilson Medical Center, Binghamton, NY; 2United Health Services, Wilson Medical Center, Johnson City, NY; 3Rochester General Hospital, Rochester, NY; 4United Health Services, Johnson City, NY Introduction: Idiopathic non-cirrhotic portal hypertension (INCPH) is a rare condition that poses a clinical diagnostic challenge. It is characterized by clinical features of portal hypertension in the absence of cirrhosis, advanced fibrosis, or thrombosis of the portal or hepatic veins. Hereby we present an atypical presentation of INCPH.
Case Description/
Methods: A 38-year-old woman with a past medical history of ITP presented with nausea and abdominal pain. Vital signs were within normal limits, and physical examination revealed right-sided abdominal tenderness and splenomegaly. Laboratory evaluation showed pancytopenia with preserved synthetic liver function and normal liver chemistries. Contrast-enhanced computed tomography (CT) and doppler ultrasound of the abdomen and pelvis confirmed patency of the portal vein, hepatic veins, and inferior vena cava. Imaging demonstrated splenomegaly, splenic and gastroesophageal varices, and umbilical vein recanalization. There was no radiologic evidence of hepatic steatosis or cirrhosis. Upper endoscopy revealed large esophageal varices without stigmata of recent bleeding. The patient was started on a non-selective beta-blocker for primary prophylaxis. Magnetic resonance imaging excluded infiltrative disease and focal hepatic lesions.
Extensive laboratory workup was done, including HIV serologies, autoimmune panels, viral hepatitis testing, myeloproliferative neoplasms (including JAK2 mutation), thrombophilia screening; all of which were unremarkable.
A transjugular liver biopsy with hepatic venography and hemodynamic assessment was performed. The hepatic vein wedge pressure was 28 mmHg, right atrial pressure was 16 mmHg, and the portosystemic gradient was 12 mmHg. The liver biopsy demonstrated preserved lobular architecture without steatosis or inflammation. Echocardiography was normal. Right heart catheterization revealed normal pulmonary artery pressures, high-normal right-sided pressures, and normal cardiac output. A bone marrow biopsy with flow cytometry was unremarkable. Discussion: This case highlights the diagnostic complexity of INCPH despite an extensive evaluation. INCPH has been associated with immunologic disorders, prothrombotic states, infections, medications, and genetic abnormalities. Given the known association between prothrombotic conditions and INCPH alongside an unrevealing workup in this patient, we hypothesize a potential link between ITP and INCPH. However, further studies are needed to explore this relationship and guide clinical management.
Figure: Computed Tomography Triple Phase Abdomen: The portal vein is widely patent with extensive shunting within the upper abdomen.
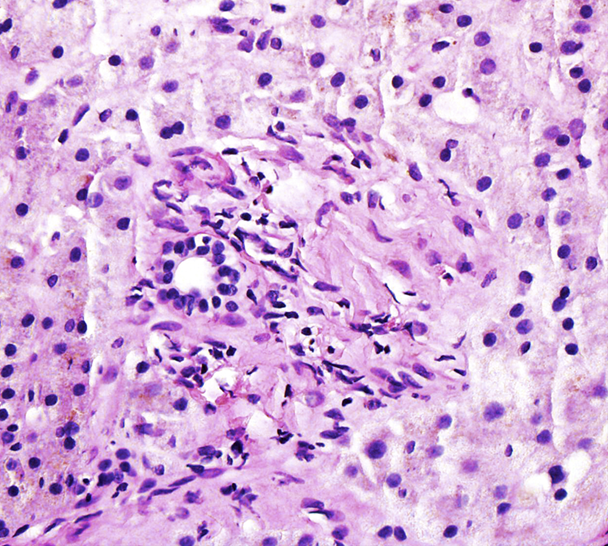
Figure: Liver Biopsy H&E x400 magnification: Portal Triad in the center surrounded by lobular tissue. Normal lobular architecture with no significant steatosis or inflammation.
Disclosures: Ahmed Shehadah indicated no relevant financial relationships. Fawad Talat indicated no relevant financial relationships. AbdulSubhan Talpur indicated no relevant financial relationships. Usama Sakhawat indicated no relevant financial relationships. Alshaima Yousef indicated no relevant financial relationships. Khandokar Talib indicated no relevant financial relationships. Godson Senyondo indicated no relevant financial relationships. Chibuike Enwereuzo indicated no relevant financial relationships. Toseef Javaid indicated no relevant financial relationships. Amanke Oranu indicated no relevant financial relationships.
Ahmed Shehadah, MD1, Fawad Talat, MD1, AbdulSubhan Talpur, MD1, Usama Sakhawat, MD2, Alshaima Yousef, MD3, Khandokar Talib, MD4, Godson Senyondo, MD1, Chibuike Enwereuzo, MD1, Toseef Javaid, MD2, Amanke Oranu, MD1. P6127 - Idiopathic Non-Cirrhotic Portal Hypertension: A Rare Case and Diagnostic Challenge, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")