SHSU College of Osteopathic Medicine San Antonio, TX
Minahil Akbar, BS1, Alia Nazarullah, MD2, Owais Syed, MD2 1SHSU College of Osteopathic Medicine, San Antonio, TX; 2University of Texas Health San Antonio, San Antonio, TX Introduction: PALB2 mutation is an uncommon, inherited, autosomal dominant mutation typically associated with increased risk of breast cancer, pancreatic cancer and ovarian, but not typically hepatocellular carcinoma. We present a complex case of advanced hepatocellular carcinoma with no known history of liver disease and known PALB2 mutation.
Case Description/
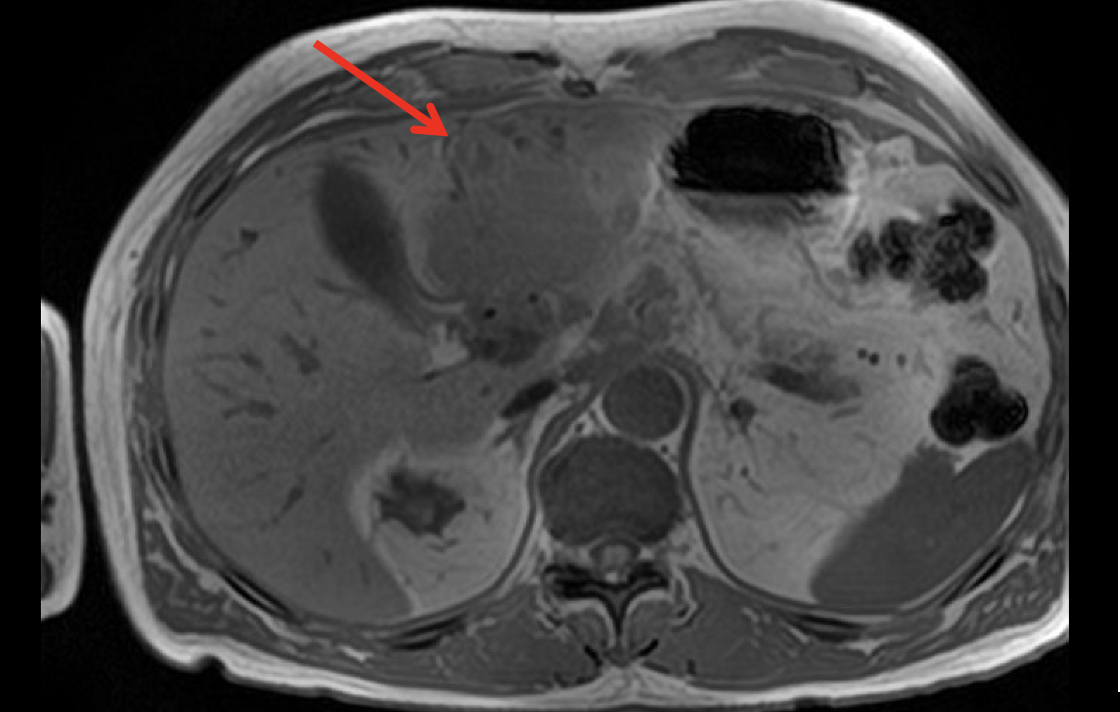
Methods: A 65-year-old male with known PALB2 mutation with negative EUS for pancreatic cancer 1.5 year prior presented for obstructive jaundice after recent identification of a left hepatic mass and proximal hepatic duct stent placement. Bilirubin was 9.4 mg/dL and alkaline phosphatase was 1476 U/L. MRCP identified a 9 cm segment 2/3 hepatic mass, right hepatic duct dilation and right internal mammary lymph node concerning for metastatic disease (figure 1). ERCP was completed with dilation and placement of stent in the right hepatic duct. Lymph node biopsy revealed CAM5.2, HepPar 1 and Arginase staining concerning poorly differentiated hepatocellular carcinoma (figure 2). Patient was referred to oncology, and was enrolled in a clinical trial for immunotherapy for advanced hepatocellular carcinoma. Unfortunately, approximately two months after diagnosis, the patient course has been complicated by enlarging left hepatic mass to 12 cm causing gastric outlet obstruction secondary to infiltration of the anterior pyloric wall by the hepatic lesion, and he ultimately decided to discharge home on hospice care. Discussion: This case highlights a previously unreported association between a germline PALB2 mutation and hepatocellular carcinoma (HCC). It is most likely that defective homologous recombination due to PALB2 loss led to genomic instability and malignant transformation. This expands the spectrum of PALB2-associated malignancies beyond breast and pancreatic cancers to include HCC. Clinically, recognizing PALB2 as a possible risk factor for HCC may prompt consideration of liver surveillance in carriers and influence therapy. Notably, DNA repair deficiencies can foster an immunogenic tumor microenvironment; indeed, preclinical models of PALB2-deficient HCC demonstrate increased T-cell infiltration and improved response to PD-1 blockade. Continued research is needed to clarify the PALB2 oncogenic role beyond its traditional cancer associations and to guide targeted management strategies.
Figure: Figure 1. MRCP demonstrating a 9 cm segment 2/3 hepatic mass
Disclosures: Minahil Akbar indicated no relevant financial relationships. Alia Nazarullah indicated no relevant financial relationships. Owais Syed indicated no relevant financial relationships.
Minahil Akbar, BS1, Alia Nazarullah, MD2, Owais Syed, MD2. P6094 - Beyond Breast and Pancreas: Hepatocellular Carcinoma in a PALB2 Carrier, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.