The Ohio State University College of Medicine Columbus, OH
Cheikh Tandiang, BA1, Emmanuel Boateng, MD2, Hannah Chi, MD3, Naima Hashi, MD3, Jacob Skeans, MD3 1The Ohio State University College of Medicine, Columbus, OH; 2University of California Davis Health, Sacramento, CA; 3The Ohio State University Wexner Medical Center, Columbus, OH Introduction: Hepatic tuberculosis (HTB) is a rare form of extrapulmonary tuberculosis and is usually seen in immunocompromised patients. The majority of HTB is in the setting of miliary TB and HIV co-infection, however it can present as an isolated entity. Diagnosing HTB can be difficult due to nonspecific symptoms such as fevers, abdominal pain, and weight loss. We present an unusual case of a 26-year-old immunocompetent patient with HTB.
Case Description/
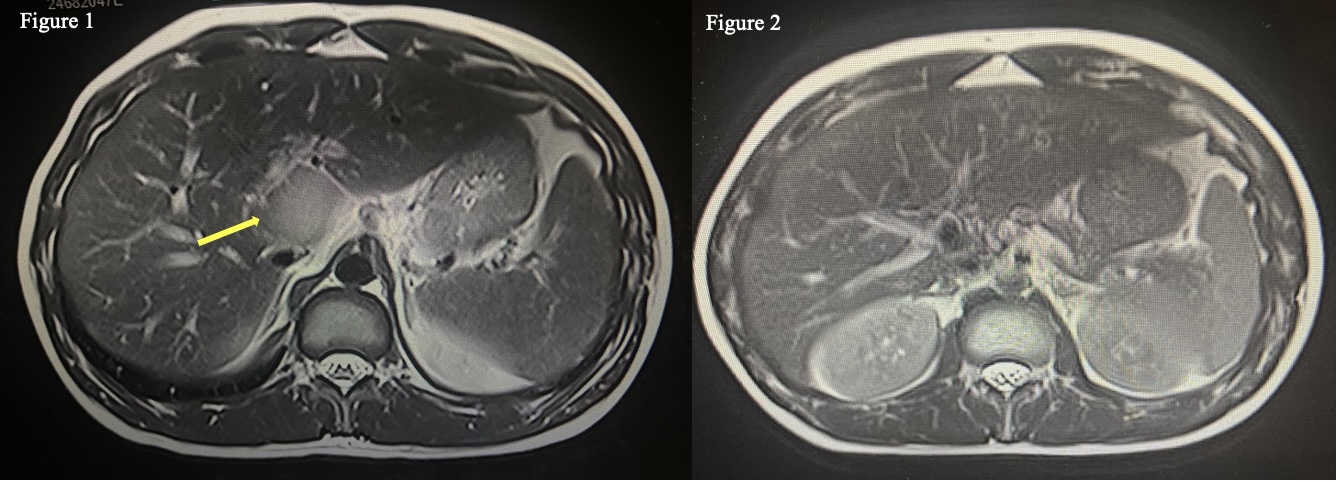
Methods: A 26-year-old male Somali immigrant presented to GI clinic with chronic abdominal pain, nausea, and loose stools. Initial work up only revealed mildly elevated CRP of 25. During his follow-up visit, he reported persistent non-productive cough, prompting TB and HIV testing. Although his HIV test was negative, he had a positive serum QuantiFERON. His CT chest showed mediastinal lymphadenopathy with multiple nodular densities in the upper left lobe consistent with reactivated TB. Abdominal CT demonstrated a 5.2 x 3.3 cm heterogenous mass in the liver, with follow-up abdominal MRI confirming the results (Figure 1). Unfortunately, the patient refused liver biopsy to rule out malignancy due to fear of sedation. Patient was initiated on RIPE therapy (rifampin, isoniazid, pyrazinamide, ethambutol).
One month after starting RIPE therapy, he developed acute worsening of his abdominal pain. Repeat abdominal MRI revealed the hepatic mass was now within the celiac plexus causing celiac compression syndrome. He agreed to undergo EUS with a liver biopsy. Pathology was negative for malignancy but demonstrated epithelioid granulomas without acid-fast bacilli, and he continued RIPE therapy for a total of 6 months. MRI after 8 months showed complete resolution of the hepatic mass (Figure 2).
Discussion: This case highlights the clinical and diagnostic challenges associated with hepatic tuberculosis, emphasizing the importance of considering it in the differential diagnosis for patients with unexplained liver lesions, particularly in regions with high TB prevalence. The incidence of TB cases in the United States has been increasing for multiple reasons such as rising use of biologics, chemotherapy and immigration of individuals from high endemic regions. HIV co-infection is also common with HTB, so the presence of HTB without HIV is rare. Diagnosis of hepatic TB can be challenging due to its non-specific clinical features and radiographic characteristics that mimic liver abscess and malignancy. Definitive diagnosis requires liver biopsy showing caseating granulomas.
Figure: Figure 1: Abdominal Magnetic Resonance Image confirming 5.2 x 3.3 cm heterogenous mass in the liver.
Figure 2: Abdominal Magnetic Resonance Image showing complete resolution of hepatic mass
Disclosures: Cheikh Tandiang indicated no relevant financial relationships. Emmanuel Boateng indicated no relevant financial relationships. Hannah Chi indicated no relevant financial relationships. Naima Hashi indicated no relevant financial relationships. Jacob Skeans indicated no relevant financial relationships.
Cheikh Tandiang, BA1, Emmanuel Boateng, MD2, Hannah Chi, MD3, Naima Hashi, MD3, Jacob Skeans, MD3. P6090 - A Rare Case of Hepatic Tuberculosis in an Immunocompetent Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")