Abdelhaleem Sideeg, MD1, Ayman Elawad, MD2, Mohammad Adam, MD, MSc3, Ali Osman, MD, MSCI Candidate4, Asma Siddique, MD5 1virginia mason medical center, Seattle, WA; 2Massachusetts General Hospital, Boston, MA; 3University of Missouri - Kansas City School of Medicine, Kansas City, MO; 4Washington University School of Medicine in St. Louis, Ballwin, MO; 5Virginia Mason Franciscan Health, Seattle, WA Introduction: Hepatocellular carcinoma (HCC) remains the most common primary liver malignancy and a leading cause of cancer-related death. Recurrent HCC presents major treatment challenges, especially in patients with cirrhosis-related complications and contraindications to standard therapies. We report a case of multifocal recurrent HCC managed successfully with STRIDE (tremelimumab + durvalumab), highlighting its potential in complex cases.
Case Description/
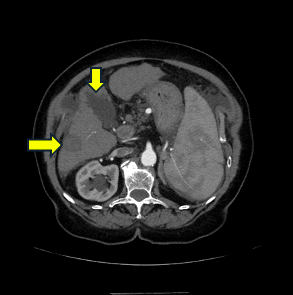
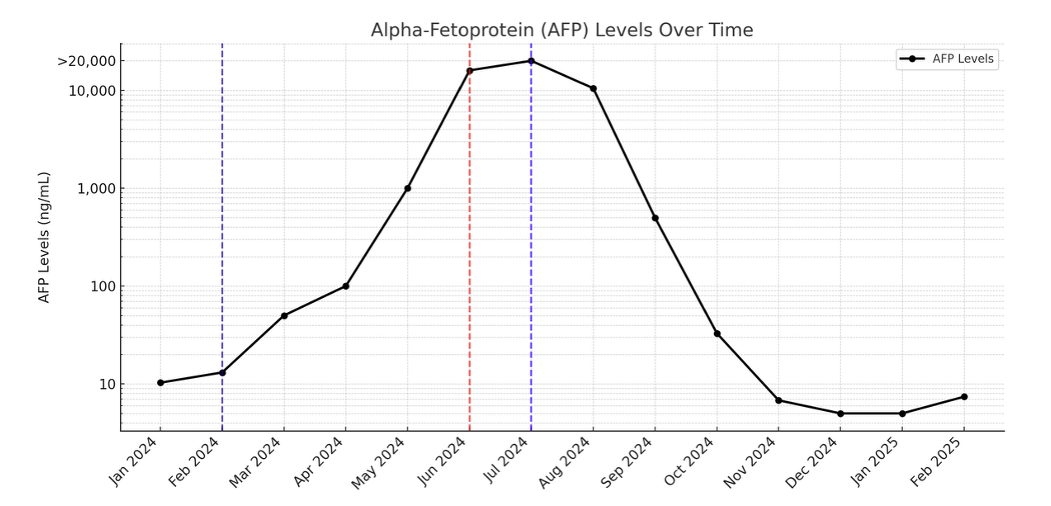
Methods: A 75-year-old woman with Child-Pugh B cirrhosis due to treated hepatitis C, portal hypertension, esophageal varices, and thrombocytopenia was undergoing routine HCC surveillance. An initial ultrasound showed a 1.1 cm lesion in segment 3. AFP was 8.2 ng/mL, and liver function was compensated. MRI confirmed a 21 x 13 mm hyperenhancing mass in segments 2–3 (LR-4); and biopsy revealed poorly differentiated HCC. Staging showed no metastasis. Due to tumor size and high surgical risk, the multidisciplinary tumor board (MDTB) recommended microwave ablation (MWA), which she underwent. At 9-month surveillance, CT showed a new 1.2 cm LR-5 lesion in segment 6. AFP increased to 96 ng/mL. Repeat MWA was performed. Nine months later, surveillance CT showed at least seven new arterial-enhancing lesions (LR-4 to LR-5) across multiple segments and an enlarged perigastric lymph node concerning for metastasis. AFP surged to >20,000 ng/mL. Given contraindications to bevacizumab (varices, thrombocytopenia), the MDTB recommended STRIDE therapy. The patient tolerated STRIDE well. At 3-month imaging, significant tumor regression was noted (Figure1), including resolution of the perigastric nodule. AFP dropped to 498.9 ng/mL at two months and 32.9 ng/mL at three months (Figure2). The patient continues to tolerate immunotherapy well. Repeat multiphasic CT scans every three months over the following nine months showed nonviable lesions with no new hepatic lesions. Discussion: HCC management includes curative options (transplant, resection, ablation) and non-curative therapies (TACE, Y-90, radiation, systemic agents). Systemic therapies recommended for patients with advanced HCC who are not candidates for resection or local regional therapy and have preserved liver function. Our case highlights the potential of the STRIDE regimen for managing recurrent multifocal metastatic HCC. It also emphasizes the role of multidisciplinary care and continued surveillance in HCC treatment strategies.
Disclosures: Abdelhaleem Sideeg indicated no relevant financial relationships. Ayman Elawad indicated no relevant financial relationships. Mohammad Adam indicated no relevant financial relationships. Ali Osman indicated no relevant financial relationships. Asma Siddique indicated no relevant financial relationships.
Abdelhaleem Sideeg, MD1, Ayman Elawad, MD2, Mohammad Adam, MD, MSc3, Ali Osman, MD, MSCI Candidate4, Asma Siddique, MD5. P6089 - Immunotherapy Breakthrough in Recurrent Metastatic Hepatocellular Carcinoma: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.