P6081 - A Strategy Utilizing Tocilizumab, Budesonide, and Mycophenolate Mofetil in the Peri-Operative Period to Achieve Biochemical Remission in High-Grade Immune Checkpoint Inhibitor-Mediated Cholangiohepatitis: A Case Study
University of Texas MD Anderson Cancer Center Houston, TX
Hao Chi Zhang, MD University of Texas MD Anderson Cancer Center, Houston, TX Introduction: About one-third of patients who develop high-grade immune-mediated hepatobiliary toxicity (IMH) induced by immune checkpoint inhibitors (ICI) may exhibit steroid-refractoriness requiring escalation of treatment. Some cases with a cholestatic component of liver injury, associated with anti-PD-1 inhibitor therapy, can exhibit suboptimal response to systemic corticosteroids alone. Emerging clinical experience has shown that tocilizumab, an IL-6 receptor antagonist, is a viable adjunctive treatment option. We present a case of ICI-mediated cholangiohepatitis (IMCH) with steroid-dependence successfully treated with tocilizumab combined with mycophenolate mofetil (MMF).
Case Description/
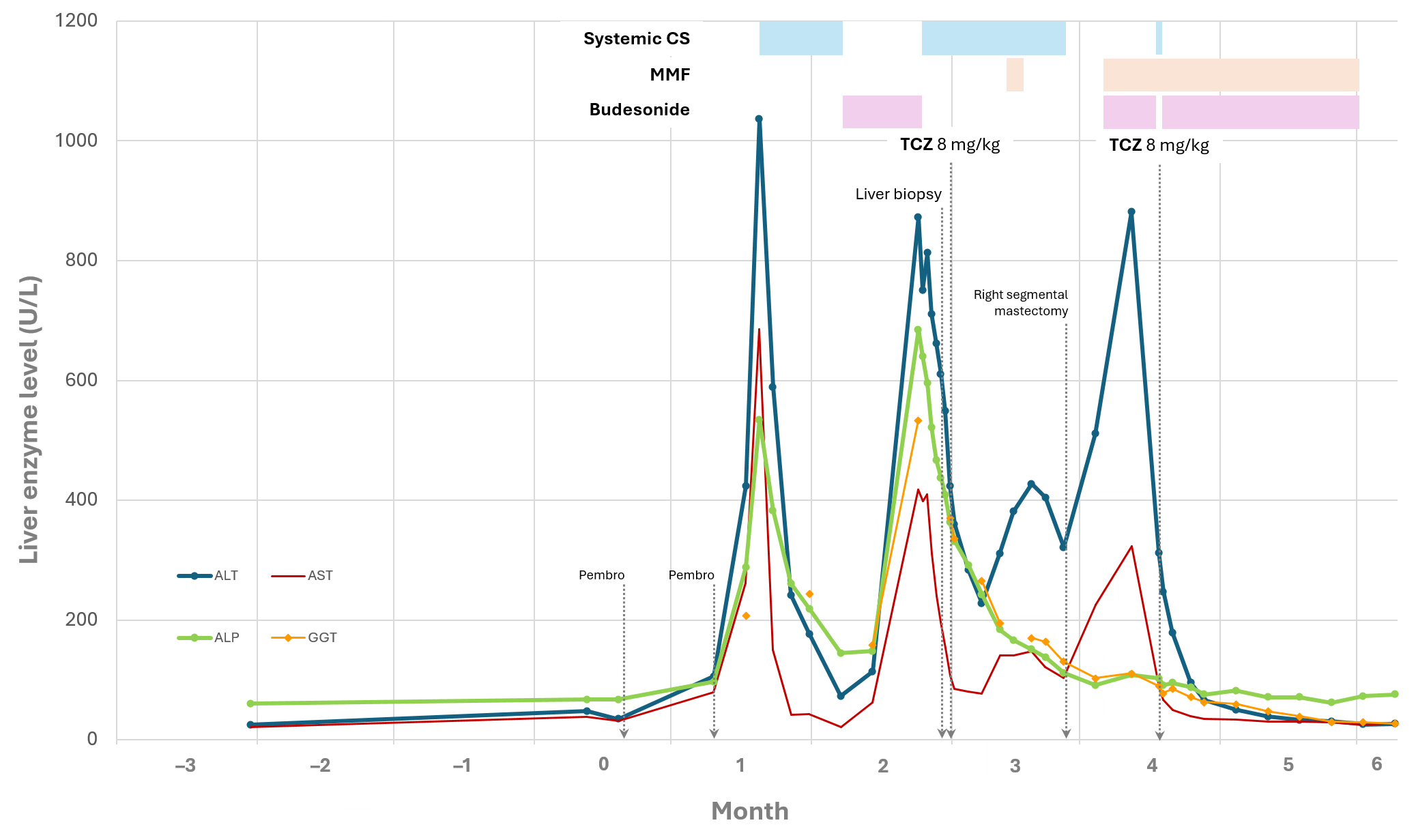
Methods: A 53-year-old woman with a history of right breast cancer treated with neoadjuvant carboplatin/paclitaxel and an ICI, pembrolizumab, developed new-onset CTCAE grade 4 liver injury. After 2 cycles of pembrolizumab, her liver enzymes increased to initial peak ALT 1,037 U/L, AST 686 U/L, and ALP 534 U/L, without liver synthetic dysfunction. Although liver enzymes initially improved after starting oral prednisone 100 mg/d (1.8 mg/kg/d) for 4 days and 75 mg/d (1.4 mg/kg/d), across 2 weeks, attempted taper to oral budesonide 9 mg/d led to resurgence of ALT to 873 U/L. After diagnostic liver biopsy confirmed IMCH, induction IV methylprednisolone (MP) 60 mg/d and IV tocilizumab (TCZ) 8 mg/kg were administered, but subsequent prednisone taper did not yield remission. Due to necessity of right segmental mastectomy, high-dose steroids were avoided peri-operatively. A week post-surgery, MMF and budesonide 9 mg/d were initiated, followed by IV MP re-induction and IV TCZ 8 mg/kg, without adverse events. After 2 weeks of budesonide 6 mg/d and 2 weeks of 3 mg/d, with cessation of MMF, she achieved complete and sustained biochemical remission. Discussion: Society guidance documents have proposed a variety of steroid-sparing adjunctive treatment options for managing steroid-refractory/steroid-dependent IMH, and TCZ has emerged as an attractive option. Use of TCZ can free a patient from steroid-dependency. One or 2 total infusions of TCZ is sufficient. We predicted that our patient would develop a protracted course of immunosuppressive need and steroid-refractoriness based on the phenotype (IMCH), prompting utilization of TCZ; MMF acted as a simultaneous bridge from systemic steroids. We also favored budesonide over prednisone to decrease the cumulative exposure to systemic steroids, especially in the peri-operative period.
Figure: Figure 1. Chronological trends of liver biochemistries with respect to the clinical course and treatments administered. Month #1 was defined as the month during which initial peak CTCAE grade 4 ALT level manifested. Intravenous (IV) induction systemic corticosteroids (methylprednisolone) was administered at both encounters for intravenous tocilizumab (TCZ) infusion. Due to the patient's planned surgery (mastectomy), deemed important for her cancer treatment, prednisone was initially tapered off, and a few days of mycophenolate mofetil (MMF) was started but soon held for a week pre-operatively. The patient was allowed to proceed with surgery despite not yet being in biochemical remission, as her ALT had not yet reached CTCAE grade 1. One week after surgery, MMF was restarted with oral budesonide. Despite this combination treatment, the ALT was noted to rise again, so a second infusion of TCZ was given, followed by budesonide of 9 mg/d until ALT approached 2x upper limit of normal, and a total 4-week taper of budesonide was prescribed. MMF was completed the same day as her last day of budesonide (3 mg). The patient achieved biochemical remission after 4 weeks after the second infusion of TCZ. She continued to exhibit sustained remission off steroids. Of note, although ursodeoxycholic acid was initially prescribed for the patient, she experienced gastrointestinal intolerance while taking it, so it was not utilized for the majority of the treatment course. Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; GGT, gamma-glutamyl transferase; CS, corticosteroids; MMF, mycophenolate mofetil; Pembro, pembrolizumab; TCZ, tocilizumab
Disclosures: Hao Chi Zhang indicated no relevant financial relationships.
Hao Chi Zhang, MD. P6081 - A Strategy Utilizing Tocilizumab, Budesonide, and Mycophenolate Mofetil in the Peri-Operative Period to Achieve Biochemical Remission in High-Grade Immune Checkpoint Inhibitor-Mediated Cholangiohepatitis: A Case Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")