Creighton University School of Medicine Phoenix, Arizona
Vishnu Yanamaladoddi, MD, Nadia Kohler, Vikash Kumar, MD, Adam J. Gomez, MD, Justin Reynolds, MD, Nilofar Najafian, MD Creighton University School of Medicine, Phoenix, AZ Introduction: Stauffer syndrome is a paraneoplastic syndrome characterized by cholestatic hepatitis in absence of intrinsic and extrinsic liver disease. First described in renal cell carcinoma (RCC), the pathophysiology is unclear. Of the cholestatic variants, the icteric form is most rare. Though classically associated with RCC, cases have been reported with other malignancies. We present a rare case of Stauffer syndrome in a patient with metastatic prostate adenocarcinoma.
Case Description/
Methods: A 70-year-old man with asthma presented with jaundice, acholic stools, 20-pound weight loss, and urinary hesitancy for several weeks. Given concern for drug-induced liver injury, tadalafil and atorvastatin were stopped, but jaundice worsened. He denied herbal or dietary supplement use.
On exam, he had jaundice, scleral icterus, pedal edema, and a facial rash. Labs showed total bilirubin 22.5 mg/dL, direct bilirubin 18.7 mg/dL, ALP 1027 U/L, GGT 70 U/L, ALT 57 U/L, and AST 73 U/L. Serologic evaluation was negative for hepatitis B/C and autoimmune markers including ANA, AMA, and anti-glycoprotein.
Ultrasound showed cholelithiasis without cholecystitis or choledocholithiasis. CT abdomen revealed no pancreatic lesions but extensive retroperitoneal, parailiac, and aortocaval lymphadenopathy, hepatomegaly, mild splenomegaly, and a markedly enlarged prostate with abnormal contour. PSA was >5000 U/L.
EUS showed normal pancreatic architecture and ducts, a collapsed 4.7 mm CBD, and multiple enlarged hypoechoic lymph nodes. Liver parenchyma showed scattered hyperechogenic lines suggestive of infiltrative disease. Lymph node biopsy confirmed metastatic prostate adenocarcinoma. Liver biopsy showed severe cholestatic hepatitis with centrilobular sinusoidal dilation without significant fibrosis.
He was diagnosed with metastatic prostate adenocarcinoma with paraneoplastic cholestatic hepatitis. Leuprolide was started for androgen deprivation and ursodeoxycholic acid for symptomatic relief. Over weeks, his jaundice and liver function significantly improved. Discussion: This case highlights an unusual presentation of metastatic prostatic adenocarcinoma manifesting as paraneoplastic cholestatic hepatitis. Though a diagnosis of exclusion, paraneoplasia should be considered in cases of unexplained cholestasis in patients with malignancies. Early recognition is critical as appropriate oncologic management can lead to resolution of hepatic dysfunction and improved patient outcomes.
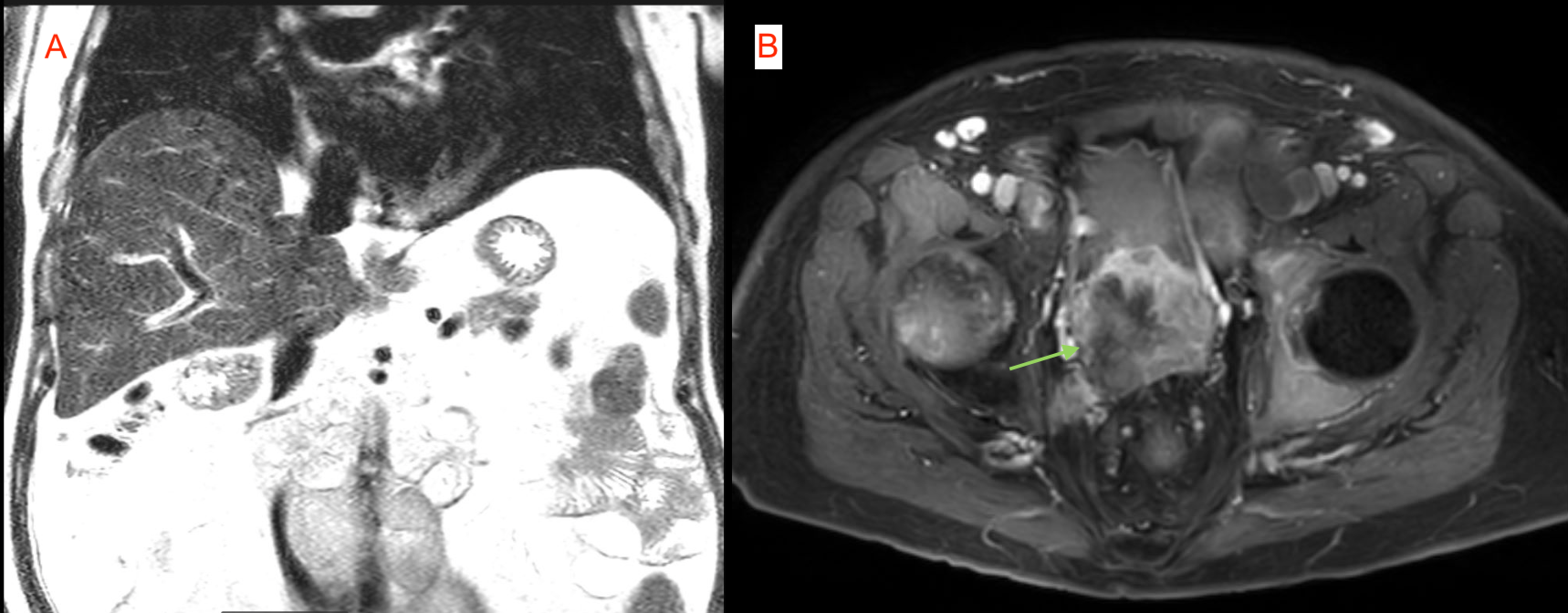
Figure: 1A - MRI showing normal liver architecture without enlargement or lesions 1B - MRI showing prostate concerning for malignancy
Figure: Liver biopsy showing cholestatic pattern of hepatitis
Disclosures: Vishnu Yanamaladoddi indicated no relevant financial relationships. Nadia Kohler indicated no relevant financial relationships. Vikash Kumar indicated no relevant financial relationships. Adam Gomez indicated no relevant financial relationships. Justin Reynolds indicated no relevant financial relationships. Nilofar Najafian indicated no relevant financial relationships.
Vishnu Yanamaladoddi, MD, Nadia Kohler, Vikash Kumar, MD, Adam J. Gomez, MD, Justin Reynolds, MD, Nilofar Najafian, MD. P6076 - Paraneoplastic Cholestatic Hepatitis in Prostate Cancer: A Rare Presentation of Stauffer Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.