Englewood Hospital and Medical Center Englewood, NJ
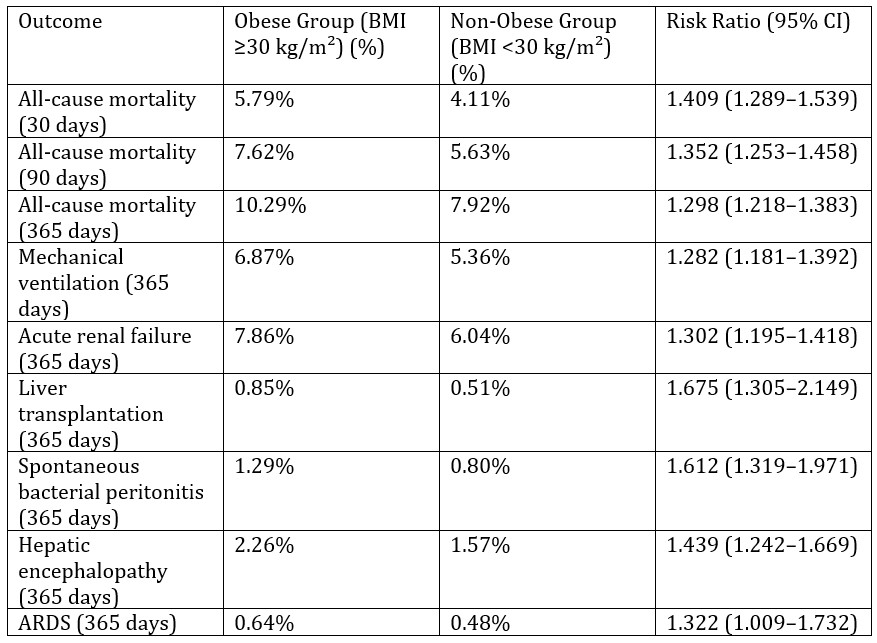
Shalva Eliava, MD1, Esraa Mohamed, MD1, Ayman Elnail, MD1, Ellen Choi, MD1, Nino Gudushauri, MD2, Irakli Tskhakaia, MD3 1Englewood Hospital and Medical Center, Englewood, NJ; 2Einstein Healthcare Network, Philadelphia, PA; 3Einstein Healthcare Network, Philadephia, PA Introduction: Alcoholic hepatitis (AH) is a severe form of alcohol-related liver disease associated with high short- and long-term mortality. Despite obesity being a prevalent and rising global comorbidity, its impact on AH remains poorly explored. This retrospective cohort study examines the relationship between obesity and clinical outcomes in patients with AH, providing insights into how this prevalent comorbidity affects mortality. Methods: Using the TriNetX network of electronic health records from 97 global healthcare organizations, we identified patients aged 18–100 diagnosed with AH. Cohorts were stratified by body mass index (BMI ≥30 kg/m² for obese and < 30 kg/m² for non-obese), identified via ICD-10 codes. Before matching, the obese cohort included 19,592 patients and the non-obese cohort 37,458. Mean age and demographics were similar (48.2 ± 12.4 vs. 47.7 ± 13 years, predominantly white males). 1:1 propensity score matching was performed for age, sex, race/ethnicity, hypertension, hyperlipidemia, diabetes mellitus, ischemic heart disease, chronic kidney disease, nicotine use, and corticosteroid use. Patients with a history of liver cell carcinoma, hepatitis B and C, cirrhosis of any etiology, acute and subacute liver failure, liver transplantation, autoimmune hepatitis, Metabolic Dysfunction-Associated Steatotic Liver Disease, and pregnancy were excluded. The primary outcome was all-cause mortality at 30, 90, and 365 days. Secondary outcomes included acute renal failure (ARF), hepatic encephalopathy (HE), spontaneous bacterial peritonitis (SBP), ARDS, mechanical ventilation, and liver transplant at 1 year. Patients with outcomes documented prior to AH diagnosis were excluded. Results: After matching, each cohort included 19,421 patients. Obesity was associated with increased mortality at all timepoints and higher rates of all secondary outcomes (Table 1). Discussion: These findings suggest that obesity independently contributes to worse clinical outcomes in patients with AH. Prospective studies are mandatory to validate these findings and optimize management strategies for obese patients with AH.
Figure: Table 1. Comparison of mortality and clinical outcomes between obese and non-obese patients with alcoholic hepatitis
Disclosures: Shalva Eliava indicated no relevant financial relationships. Esraa Mohamed indicated no relevant financial relationships. Ayman Elnail indicated no relevant financial relationships. Ellen Choi indicated no relevant financial relationships. Nino Gudushauri indicated no relevant financial relationships. Irakli Tskhakaia indicated no relevant financial relationships.
Shalva Eliava, MD1, Esraa Mohamed, MD1, Ayman Elnail, MD1, Ellen Choi, MD1, Nino Gudushauri, MD2, Irakli Tskhakaia, MD3. P3695 - Impact of Obesity on Mortality and Clinical Outcomes in Patients With Alcoholic Hepatitis: A Retrospective Matched Cohort Analysis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.