Samuel Schachter, MD, Nicholas McDonald, MD Temple University, Philadelphia, PA Introduction: Endoscopic ultrasound-guided fine-needle biopsy (EUS-FNB) is a commonly used diagnostic tool for evaluation and biopsy of luminal lesions or adjacent structures. Here, we present a case of a recurrent thyroid mass in a patient with prior papillary thyroid carcinoma suspicious for recurrent disease in the surgical bed, with limited other options for biopsy. In this case, the patient underwent EUS-FNB of the inferior thyroid surgical resection bed with a final diagnosis of recurrent papillary thyroid carcinoma.
Case Description/
Methods: A 54-year-old man had been incidentally found to have a thyroid mass after imaging following a motor vehicle collision. Evaluation revealed T1bN1a papillary thyroid cancer and he ultimately required total thyroidectomy, right central neck dissection, and post-resection radioactive iodine therapy later that year. Less than a year later, he was found to have rising thyroglobulin levels and repeat imaging revealed a 23 mm x 14 mm right paratracheal mass in the inferior aspect of the surgical resection bed (Figure 1). The patient underwent evaluation at multidisciplinary tumor board with ENT, thoracic surgery, interventional radiology and interventional pulmonology. Given that the mass was deep to the aorta and in proximity to the carotid and innominate arteries, there was felt to be no safe window for mediastinoscopy with biopsy, percutaneous biopsy or endobronchial ultrasound. The risk for repeat surgical biopsy by ENT was felt to be extremely high given surgical history and the patient had a strong desire to avoid surgery.
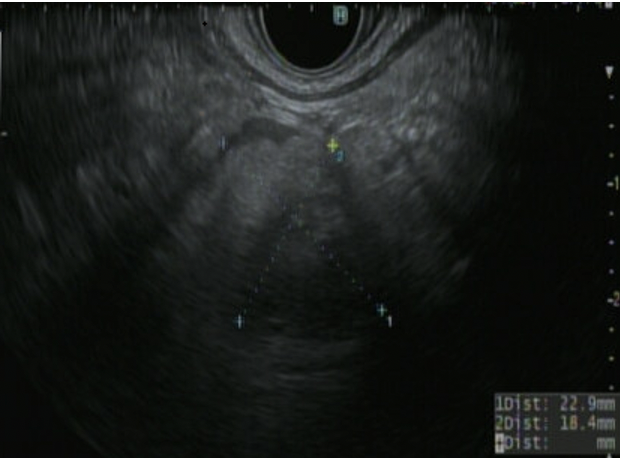
Therefore, the patient was referred to Interventional Gastroenterology to attempt EUS-FNB, and identify the lesion from the proximal esophagus from a safe window. After discussing risks and benefits, the patient underwent EUS, revealing a 20 x 16 mm mediastinal, hypoechoic, heterogenous mass in the suspected thyroid surgical bed (Figure 2). After using color doppler to avoid vascular structures, FNB was obtained with three passes using a 25-gauge needle. Pathology exhibited follicular cells in papillary arrangements with nuclear enlargement, intranuclear inclusions, and grooves consistent with papillary thyroid carcinoma. Discussion: While there are several available options for mediastinal biopsy, at times anatomic considerations may make conventional approaches not feasible. While limited data exist for EUS-FNB of the thyroid, endoscopic ultrasound can be considered in these difficult cases after multidisciplinary discussion.
Figure: Mediastinal mass seen on computed tomography scan of the neck
Figure: Hypoechoic mass seen endosonographically
Disclosures: Samuel Schachter indicated no relevant financial relationships. Nicholas McDonald indicated no relevant financial relationships.
Samuel Schachter, MD, Nicholas McDonald, MD. P3620 - Endoscopic Ultrasound Fine Needle Biopsy in Diagnosis of High-Risk Metastasis of Papillary Thyroid Cancer, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")