Department of Medicine, George Washington University School of Medicine and Health Sciences Washington, DC
Zeina Bani Hani, MBBS1, Romy Chamoun, MD2, Simran Gupta, MD3, Jennie Zhang, DO2, Marie L. Borum, MD, EdD, MPH, FACG3, Hemanth Gavini, MD, MPH3 1Department of Medicine, George Washington University School of Medicine and Health Sciences, Washington, DC; 2George Washington University, Washington, DC; 3Division of Gastroenterology and Liver Disease, Department of Medicine, George Washington University School of Medicine and Health Sciences, Washington, DC Introduction: Duodenal narrowing can lead to obstruction of the passage of gastrointestinal contents. This narrowing may be caused by intrinsic factors such as benign or malignant tumors, peptic ulcer disease (PUD), inflammatory bowel disease, or extrinsic compression. The most common malignancies causing bowel obstruction include colon, stomach, and ovarian. Rarely, metastases from extra-abdominal cancers cause duodenal obstruction. We report an unusual case of metastatic bladder cancer causing duodenal obstruction.
Case Description/
Methods: An 82-year-old male with hypertension, atrial flutter, and bladder cancer (diagnosed 2 years prior) treated with transurethral resection and concurrent chemoradiation presented with persistent nausea and vomiting. Surveillance cystoscopy revealed no evidence of local recurrence of bladder cancer. An abdominal CT revealed a distended stomach and duodenum, and a duodenal diverticulum. An Esophagogastroduodenoscopy (EGD)showed esophagitis with ulcer and significant residue in the stomach and duodenum. Magnetic Resonance Enterography (MRE) revealed smooth stenosis in the 3rd duodenal segment resulting in obstruction of the duodenum, without evidence of any mass. A subsequent Endoscopic Ultrasound (EUS) showed thickening of the wall of the 3rdportion of the duodenum due to infiltration by an extrinsic 2-cm, ill-defined hypoechoic lesion. A fine needle biopsy of the lesion was performed . Pathology revealed urothelial carcinoma consistent with his prior malignancy. He underwent a gastrojejunostomy to bypass the obstruction and was discharged tolerating adequate oral intake. Discussion: Metastatic urothelial cancers uncommonly cause duodenal obstruction.Diagnosis is typically established through a combination of imaging modalities, such as upper gastrointestinal series, CT scan, MRE and endoscopy which can identify the site and cause of the obstruction.. EUS can improve the diagnostic yield by identifying lesions not visualized on other imaging modalities and assists with diagnosis through fine needle sampling. It is believed that progression along the retro-mesenteric plane may be the key pathway by which advanced bladder cancer results in duodenal obstruction.This case highlights a rare presentation of advanced bladder cancer and the need for heightened level of suspicion of cancer recurrence in patients with symptoms of gastrointestinal obstruction.
Figure: Endoscopic Ultrasound (EUS) showing the hypoechoic area.
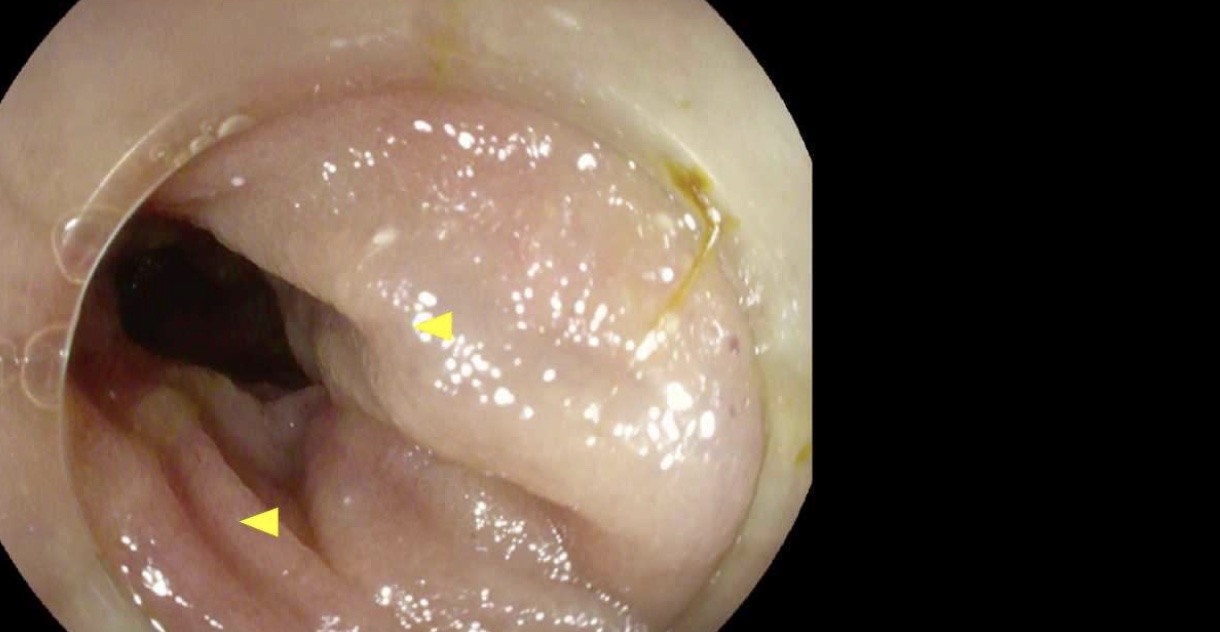
Figure: 3rd portion of the duodenum showing stenosis.
Disclosures: Zeina Bani Hani indicated no relevant financial relationships. Romy Chamoun indicated no relevant financial relationships. Simran Gupta indicated no relevant financial relationships. Jennie Zhang indicated no relevant financial relationships. Marie Borum indicated no relevant financial relationships. Hemanth Gavini indicated no relevant financial relationships.
Zeina Bani Hani, MBBS1, Romy Chamoun, MD2, Simran Gupta, MD3, Jennie Zhang, DO2, Marie L. Borum, MD, EdD, MPH, FACG3, Hemanth Gavini, MD, MPH3. P3601 - Metastatic Bladder Cancer Causing Duodenal Narrowing: A Rare Presentation of Gastrointestinal Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.