Avneet Kaur, MBBS1, Abinash Subedi, MD1, Abdelkader Chaar, MD1, Azhar Hussain, MBBS2, Bishnu Sapkota, MD, FACG1, Hafiz Muzaffar Akbar Khan, MD3 1SUNY Upstate Medical University, Syracuse, NY; 2SUNY Upstate Medical University Hospital, Syracuse, NY; 3AdventHealth, Tampa, FL Introduction: Laparoscopic cholecystectomy (LC) is the standard treatment for symptomatic cholelithiasis. A rare complication is surgical clip migration into the common bile duct, where the clip may serve as a nidus for bile stone formation. This can result in serious complications such as obstructive jaundice, cholangitis, and pancreatitis. While clip migration typically occurs within two years, delayed cases have been reported up to decades later. We present a case of choledocholithiasis secondary to clip migration, presenting eight years post cholecystectomy.
Case Description/
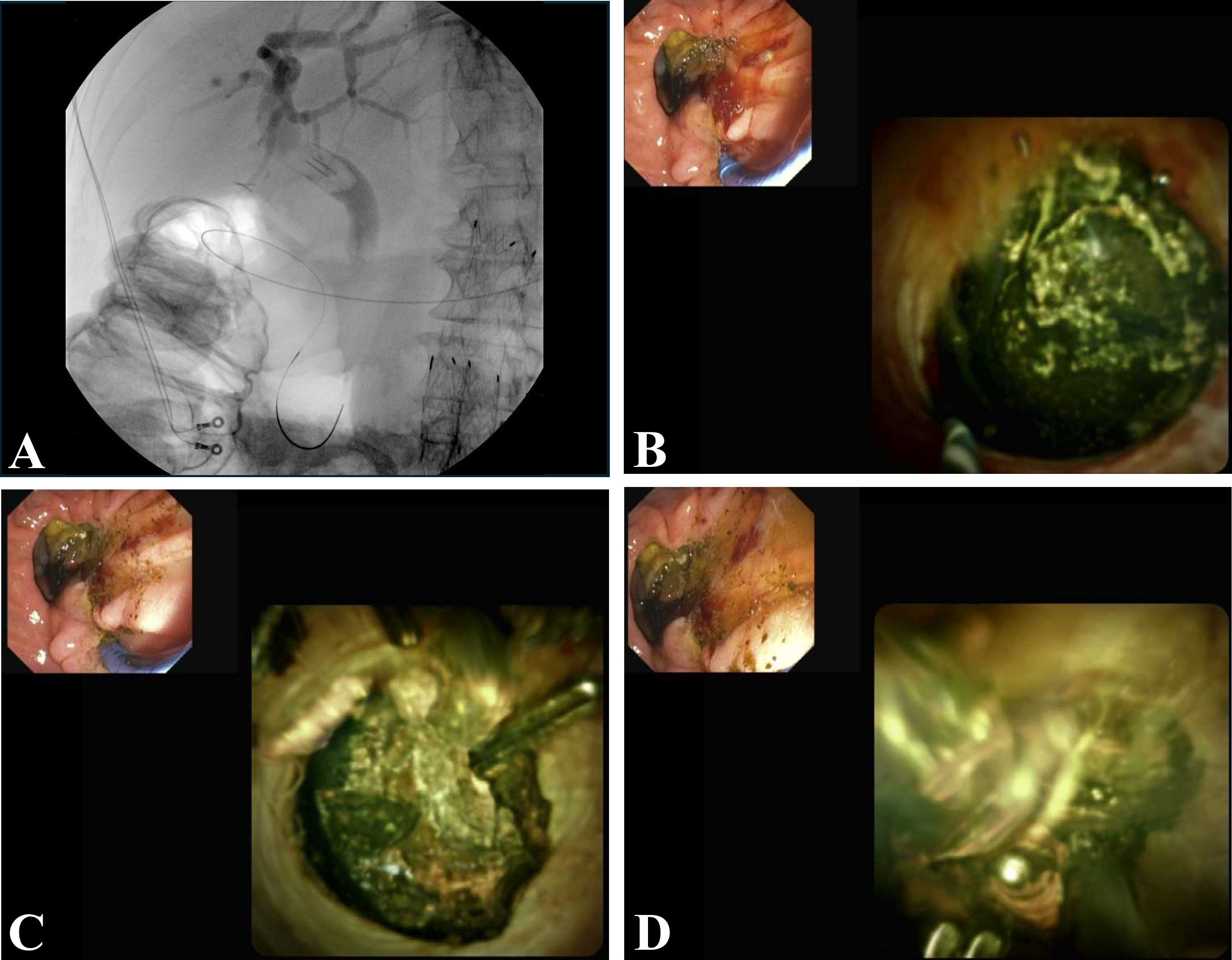
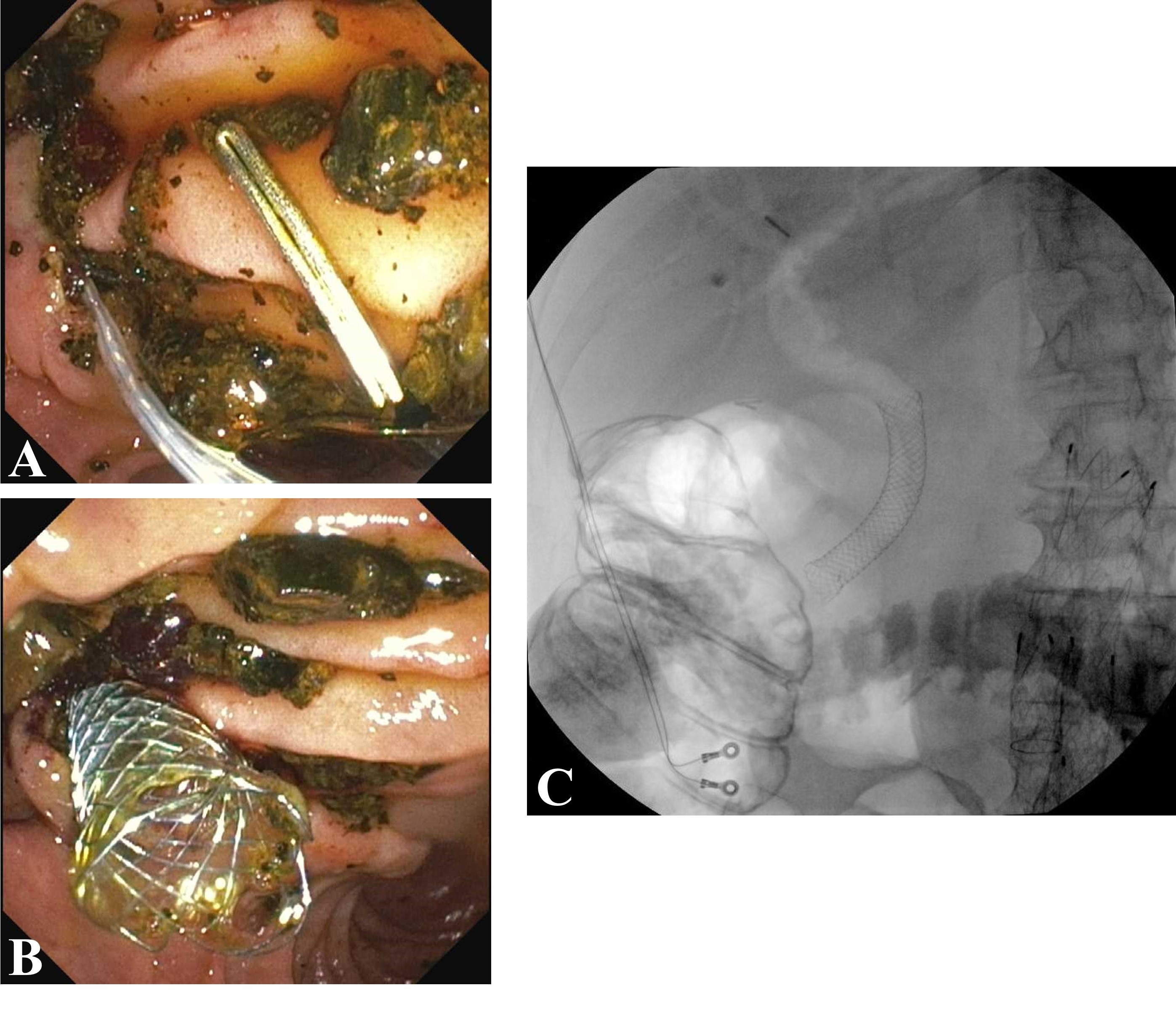
Methods: An 83-year-old male with a history of laparoscopic cholecystectomy, abdominal aortic aneurysm, and benign prostatic hyperplasia presented with abdominal pain, nausea, and vomiting following a failed endoscopic retrograde cholangiopancreatography (ERCP) at an outside hospital. Laboratory workup revealed leukocytosis (WBC 17,300/µL), elevated lipase (238 U/L), ALT 87, AST 36, alkaline phosphatase 172 U/L, and total bilirubin of 3.3 mg/dL. Abdominal imaging showed retained surgical clips. Repeat ERCP (EUS guided access as transpapillary access failed) revealed a 20 mm common bile duct stone encasing a migrated surgical clip. Electrohydraulic lithotripsy (EHL) was performed, fragmenting the stone. The biliary duct was then swept using an 11.5 mm balloon, and a 10 mm × 6 cm covered metal biliary stent was placed to maintain ductal patency and prevent bile leak. The patient’s symptoms resolved post-procedure. Discussion: This case highlights a rare but important complication of laparoscopic cholecystectomy; surgical clip migration serving as a nidus for stone formation years later. The mechanism likely involves ischemic necrosis or erosion of the cystic duct remnant, enabling clip displacement and eventual embedding within biliary concretions. Over time, this embedded foreign body can lead to clinically significant choledocholithiasis.
Symptoms often mimic typical biliary pathology, including cholangitis, jaundice, and pancreatitis, which can delay diagnosis. ERCP remains the mainstay for diagnosis and treatment. EHL is particularly effective for fragmenting large or clip-centered stones. Clinicians should be aware of clip migration post-cholecystectomy causing recurrent biliary symptoms such as cholangitis.
Figure: Figure 1: A- Fluoroscopy showing surgical clip within the bile duct with a filling defect. B- Large stone within the bile duct. C- Surgical clip seen on chonagioscopy. D- EHL stone fragment.
Figure: Figure 2 A- Clip after removal. B- Biliary stent placement. C- Fluoroscopy showing biliary stent placement after removal of stones and surgical clip.
Disclosures: Avneet Kaur indicated no relevant financial relationships. Abinash Subedi indicated no relevant financial relationships. Abdelkader Chaar indicated no relevant financial relationships. Azhar Hussain indicated no relevant financial relationships. Bishnu Sapkota indicated no relevant financial relationships. Hafiz Muzaffar Akbar Khan indicated no relevant financial relationships.
Avneet Kaur, MBBS1, Abinash Subedi, MD1, Abdelkader Chaar, MD1, Azhar Hussain, MBBS2, Bishnu Sapkota, MD, FACG1, Hafiz Muzaffar Akbar Khan, MD3. P3591 - Migrated Surgical Clip as a Nidus for Choledocholithiasis Eight Years Post-Cholecystectomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")