P3569 - Bridging the Gap: Endoscopic Deployment of a Self-Expanding Metal Stent to Relieve Descending Colon Cancer Obstruction and Avoid Diverting Colostomy
Pierce L.. Claassen, MD1, Terry L.. Jue, MD2 1Mayo Clinic, Scottsdale, AZ; 2Mayo Clinic Arizona, Scottsdale, AZ Introduction: Self-expanding metal stents (SEMS) are often used to palliate incurable malignant colon obstruction as an alternative to diverting colostomy. Surgical management of resectable left colon cancer obstruction usually requires diversion and a stoma, resection of the malignancy, and creation of a Hartmann’s pouch with potential for future revision re-anastomosis, or “takedown”. In collaboration with surgeons, endoscopists have placed SEMS to relieve left-sided colon cancer obstruction as a bridge to definitive colectomy with primary anastomosis. We illustrate a case of endoscopic stenting of descending colon adenocarcinoma to relieve obstruction and facilitate definitive, laparoscopic colectomy with primary end-to-end anastomosis at a tertiary referral center.
Case Description/
Methods: A 48-year-old man was admitted with colon obstruction after having been diagnosed with descending colorectal adenocarcinoma 4 weeks prior. Despite significant stool burden, a pediatric colonoscope was advanced to a malignant stricture in the descending colon. Fluoroscopy with luminal contrast defined the stricture. A 0.035’’ guidewire was advanced and a through-the-scope 25mm x 9mm uncovered SEMS was deployed. Copious stool passed and decompression was achieved. 10 weeks later, a laparoscopic left hemicolectomy with primary end-to-end colonic anastomosis was accomplished. Discussion: This clinical vignette highlights effective use of SEMS to decompress malignant obstruction prior to definitive oncologic resection. Studies report that using SEMS to bridge to surgery for left-sided colorectal cancer reduces short-term morbidity by lowering perforation risk and increasing odds of successful primary anastomosis. This by default also reduces the need for diverting colostomy. Moreover, Hartmann’s procedure takedown success is limited with 46% of patients being indefinitely stoma-dependent. Complications such as post-operative ileus, anastomotic leaks, strictures, and deep wound dehiscence may occur with re-anastomosis. Limitations of SEMS include access to therapeutic endoscopy as well as multi-disciplinary surgery, and oncologic care. Perforation with tumor seeding, bleeding, and SEMS migration or occlusion are inherent risks. Collaborative guidance to select patients who may benefit from SEMS to relieve left-sided malignant obstruction provides opportunities to facilitate definitive care that decreases surgery-associated morbidity and improves quality of life.
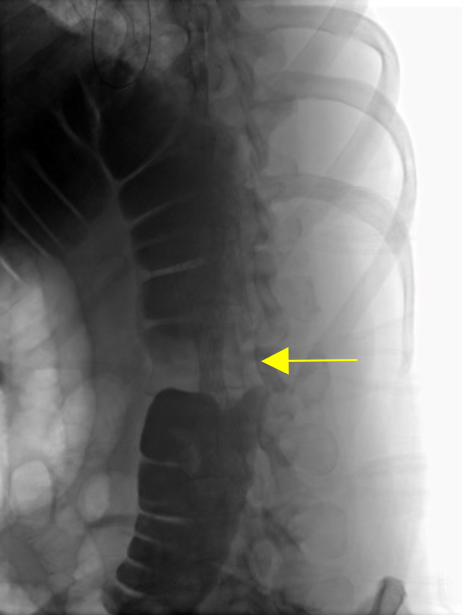
Figure: Fluoroscopic image showing the SEMS traversing a malignant stricture from a descending colon adenocarcinoma.
Figure: A photograph of the transected descending colon surgical specimen containing the adenocarcinoma with pressure-induced indentations caused by the SEMS.
Disclosures: Pierce Claassen indicated no relevant financial relationships. Terry Jue: Boston Scientific – Jan 2024, Honorarium received for serving as an Instructor at Fellows' Tissue resection course.
Pierce L.. Claassen, MD1, Terry L.. Jue, MD2. P3569 - Bridging the Gap: Endoscopic Deployment of a Self-Expanding Metal Stent to Relieve Descending Colon Cancer Obstruction and Avoid Diverting Colostomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.