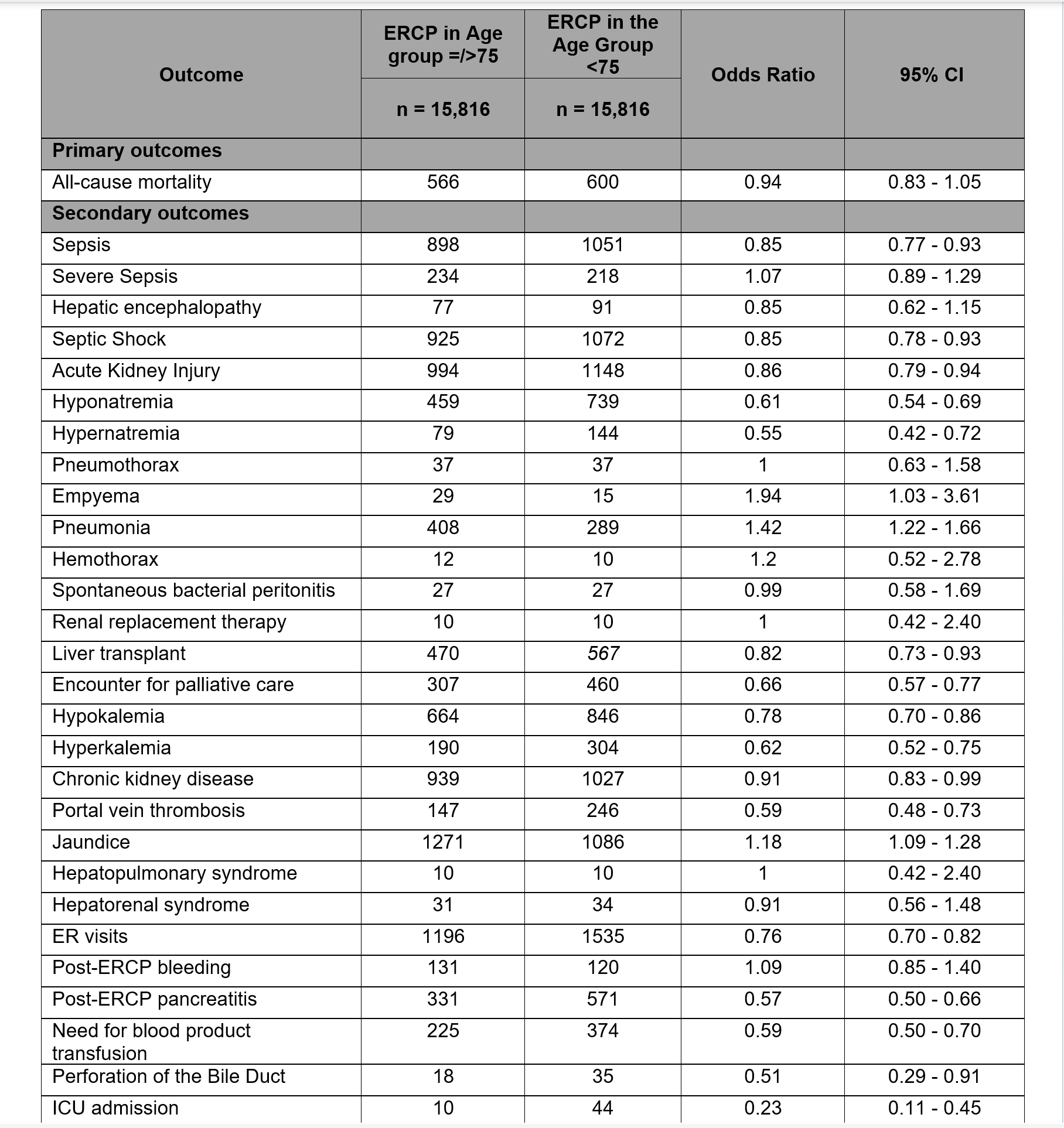
Umar Hayat, MD1, Saba Afroz, MD1, Azhar Hussain, MD2, Muhammad Kamal, MD3, Muhammad Usman Haider, MD1, Kalsoom Khalil, MD4, Wajeeh hassan, MBBS5, Aamir Saeed, MD6, Shefali Mody, MBBS2, Manesh Gangwani, MD7, Ali Siddiqui, MD8, Douglas G. Adler, MD, FACG9 1Geisinger Wyoming Valley Medical Center, Wilkes-Barre, PA; 2SUNY Upstate Medical University Hospital, Syracuse, NY; 3Hackensack Meridian Health, Edison, NJ; 4Ameer Ud Din Medical College, Syracuse, NY; 5Allama Iqbal Medical College, Lahore, Lahore, Punjab, Pakistan; 6Vanderbilt University Medical Center, Nashville, TN; 7University of Arkansas for Medical Sciences, Little Rock, AR; 8Maimonides Medical Center, Fairfax, VA; 9Center for Advanced Therapeutic (CATE), Centura Health, Porter Adventist Hospital, Peak Gastroenterology, Denver, CO Introduction: Endoscopic retrograde cholangiopancreatography (ERCP) is considered the gold standard for diagnosing and treating various hepatobiliary conditions. Nevertheless, there exists a paucity of data regarding post-ERCP complications within the elderly demographic. This study aims to investigate post-ERCP outcomes, encompassing adverse events and complications, in patients aged 75 and older. ERCP continues to be studied concerning its safety for elderly individuals. Prior studies have yielded mixed results concerning complications, frequently lacking comprehensive geriatric assessments. Methods: We conducted a retrospective, propensity-matched cohort study using data from the TriNetX research network, involving individuals aged 18 to 89 who underwent ERCP for hepatobiliary conditions. Patients were divided into two age cohorts: those under 75 years old and those 75 years and older. We used regression analysis with odds ratios to assess all-cause mortality as the primary outcome. Secondary outcomes included post-ERCP complications like sepsis, septic shock, acute kidney injury, and electrolyte imbalances, and adverse outcomes such as ICU stay, blood product infusion, and bleeding. Results: Mortality rates did not differ significantly (OR 0.94; CI 0.83–1.05) between the two groups. Older adults (aged >75 years) exhibited lower odds of developing post-ERCP pancreatitis (PEP) (OR 0.57; CI 0.50–0.66), sepsis (OR 0.85; CI 0.77–0.93), acute kidney injury (OR 0.86; CI 0.79–0.94), hyponatremia (OR 0.61; CI 0.54–0.69), and hypernatremia (OR 0.55; CI 0.42–0.72). Additionally, advanced age correlated with reduced odds of portal vein thrombosis (OR 0.59; CI 0.48–0.73), hyperkalemia (OR 0.62; CI 0.52–0.75), and hypokalemia (OR 0.78; CI 0.70–0.86). In contrast, elderly patients had higher odds of experiencing empyema (OR, 1.94; CI, 1.03–3.61), pneumonia (OR, 1.42; CI, 1.22–1.66), and jaundice (OR, 1.18; CI, 1.09–1.28). ICU admissions (OR 0.23; CI 0.11–0.45) and the need for blood transfusions (OR 0.59; CI 0.50–0.70) were significantly lower among older patients. Figure 1. Discussion: Elderly patients undergoing ERCP have a lower risk of complications, such as PEP, sepsis, and electrolyte disturbances, with mortality rates comparable to those of younger patients. However, they may experience a higher incidence of respiratory and biliary complications. These findings reinforce the safety of ERCP in older populations but underscore the need for vigilance regarding respiratory and biliary outcomes.
Figure: Primary and Secondary Outcomes in post-ERCP in two age groups
Disclosures: Umar Hayat indicated no relevant financial relationships. Saba Afroz indicated no relevant financial relationships. Azhar Hussain indicated no relevant financial relationships. Muhammad Kamal indicated no relevant financial relationships. Usman Haider indicated no relevant financial relationships. Kalsoom Khalil indicated no relevant financial relationships. Wajeeh hassan indicated no relevant financial relationships. Aamir Saeed indicated no relevant financial relationships. Shefali Mody indicated no relevant financial relationships. Manesh Gangwani indicated no relevant financial relationships. Ali Siddiqui indicated no relevant financial relationships. Douglas Adler: Boston Scientific – Consultant.
Umar Hayat, MD1, Saba Afroz, MD1, Azhar Hussain, MD2, Muhammad Kamal, MD3, Muhammad Usman Haider, MD1, Kalsoom Khalil, MD4, Wajeeh hassan, MBBS5, Aamir Saeed, MD6, Shefali Mody, MBBS2, Manesh Gangwani, MD7, Ali Siddiqui, MD8, Douglas G. Adler, MD, FACG9. P3535 - Feasibility and Safety of ERCP in the Elderly Population – A Propensity-Matched Retrospective Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.