Department of Internal Medicine, Texas Health Presbyterian Hospital Dallas, Texas Health Resources, Dallas, TX Dallas, TX
Samantha Lujan, MD1, Daniel Ellis, MD2, Diane Nguyen, MD2, Jonathan Baker, MD3 1Department of Internal Medicine, Texas Health Presbyterian Hospital Dallas, Texas Health Resources, Dallas, TX, Dallas, TX; 2Department of Internal Medicine at UT Southwestern Medical Center, Dallas, TX; 3Department of Anatomic & Clinical Pathology at Texas Health Dallas Presbyterian, Dallas, TX Introduction: Outside typical gastrointestinal or arthritic syndromes associated with Whipple’s disease (WD), there are rare instances where diffuse, chronic disease has presented as peritoneal abnormalities mimicking carcinomatosis. The nonspecific symptoms of weight loss, abdominal pain, and radiological findings can resemble malignancy. In these atypical cases, diagnosis of WD requires strong clinical suspicion and awareness of its capacity to involve serosal surfaces (pleura and peritoneum), as in our case of WD with peritoneal nodularity and right pleural effusion that mimicked disseminated disease.
Case Description/
Methods: A 61-year-old male with history of atrial flutter presented with worsening nausea, abdominal pain, and weight loss. CT abdomen showed extensive mesenteric lymphadenopathy, raising concerns for infection vs. malignancy. Exploratory laparoscopy for suspected appendicitis revealed peritoneal nodules; biopsies showed xanthogranulomatous inflammation (XGI) and mesothelial hyperplasia, with no malignancy detected. On return visit for worsening symptoms and new rash, labs revealed elevated CRP and ESR. CT chest showed a large right pleural effusion, prompting thoracentesis that found exudative fluid with no malignant cells or organisms. Given no clear etiology for weight loss and symptoms, he underwent esophagogastroduodenoscopy, which revealed PAS-positive foamy macrophages on duodenal biopsy, confirming WD. He received appropriate antibiotics and showed marked improvement at 6-month follow-up. Discussion: Serosal involvement in WD is unique, with few documented cases in the literature. Diffuse peritoneal studding, pleural effusion, and rash are patterns that rarely dominate the clinical picture of WD. One case observed an exudative, sterile pleural effusion and nodularities of the peritoneum and uterine tissue in WD. The peritoneal implants' infiltrative appearance resembles carcinomatosis, leading to confusion with malignancy. XGI and mesothelial hyperplasia may serve as histological clues to chronic WD, as reports have documented these findings on serosal surface biopsies. Although uncommon, skin manifestations of WD have been seen to include widespread macular rashes on trunk and limbs, consistent with our patient's exam, and may reflect immune dysregulation in response to systemic infection. This case highlights WD’s ability to mimic malignancy and systemic inflammation, underscoring the need for early inclusion in the differential for unexplained wasting and serosal involvement.
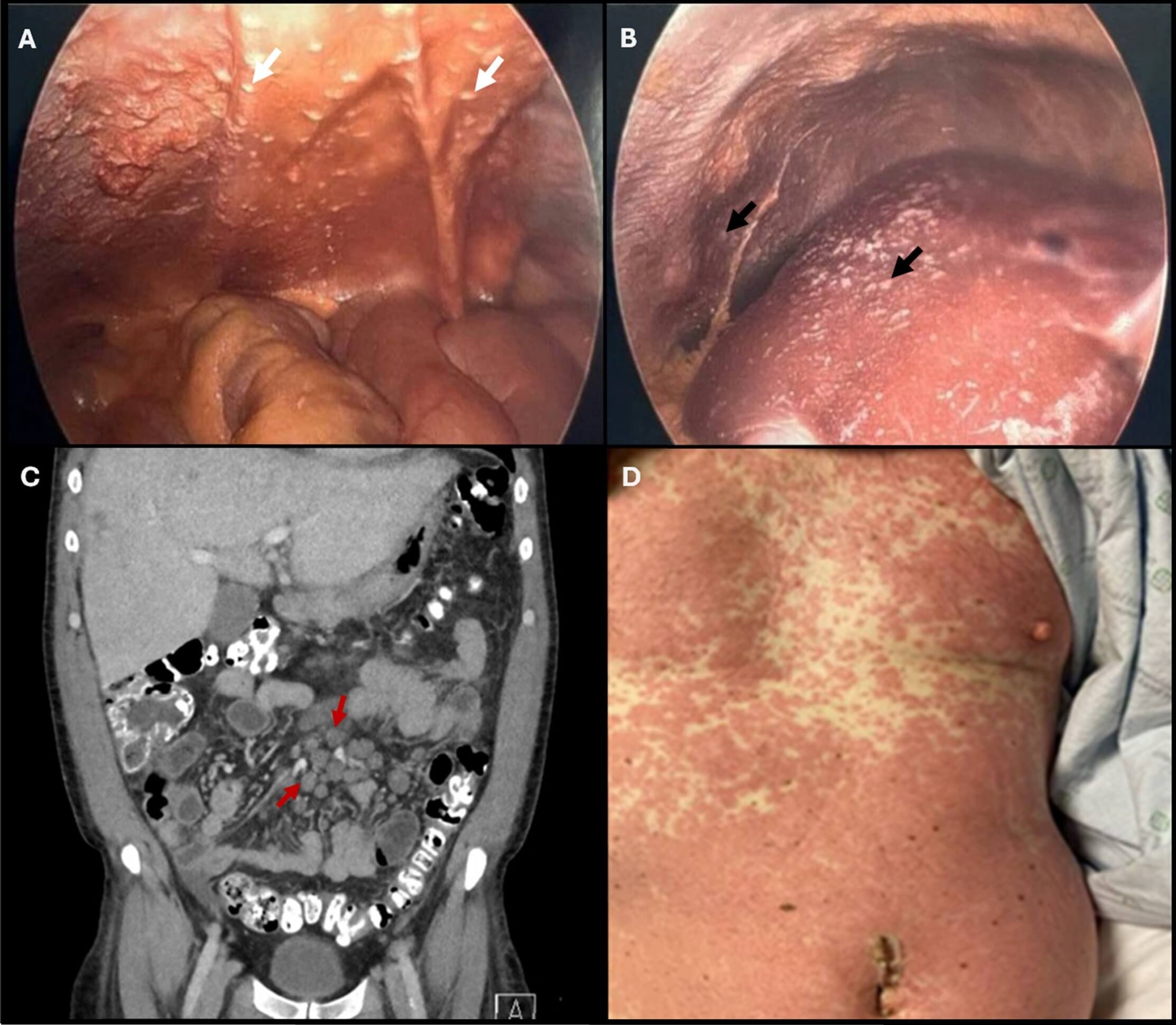
Figure: Figure 1. (A) Scattered peritoneal nodularities are visualized intraoperatively (white arrows). (B) Irregular whitish plaques (black arrow) are seen on the hepatic surface. The distribution and gross appearance raised concern for peritoneal carcinomatosis of unclear primary origin. (C) Coronal CT image demonstrating prominent, clustered lymph nodes throughout the small bowel mesentery (red arrows). (D) Clinical image of the abdomen showing a widespread, symmetric, erythematous eruption characterized by confluent pink-to-red macules and papules. The rash recurred following an initial treatment period and may represent a systemic inflammatory manifestation of Whipple’s disease—a rarely reported cutaneous phenotype.
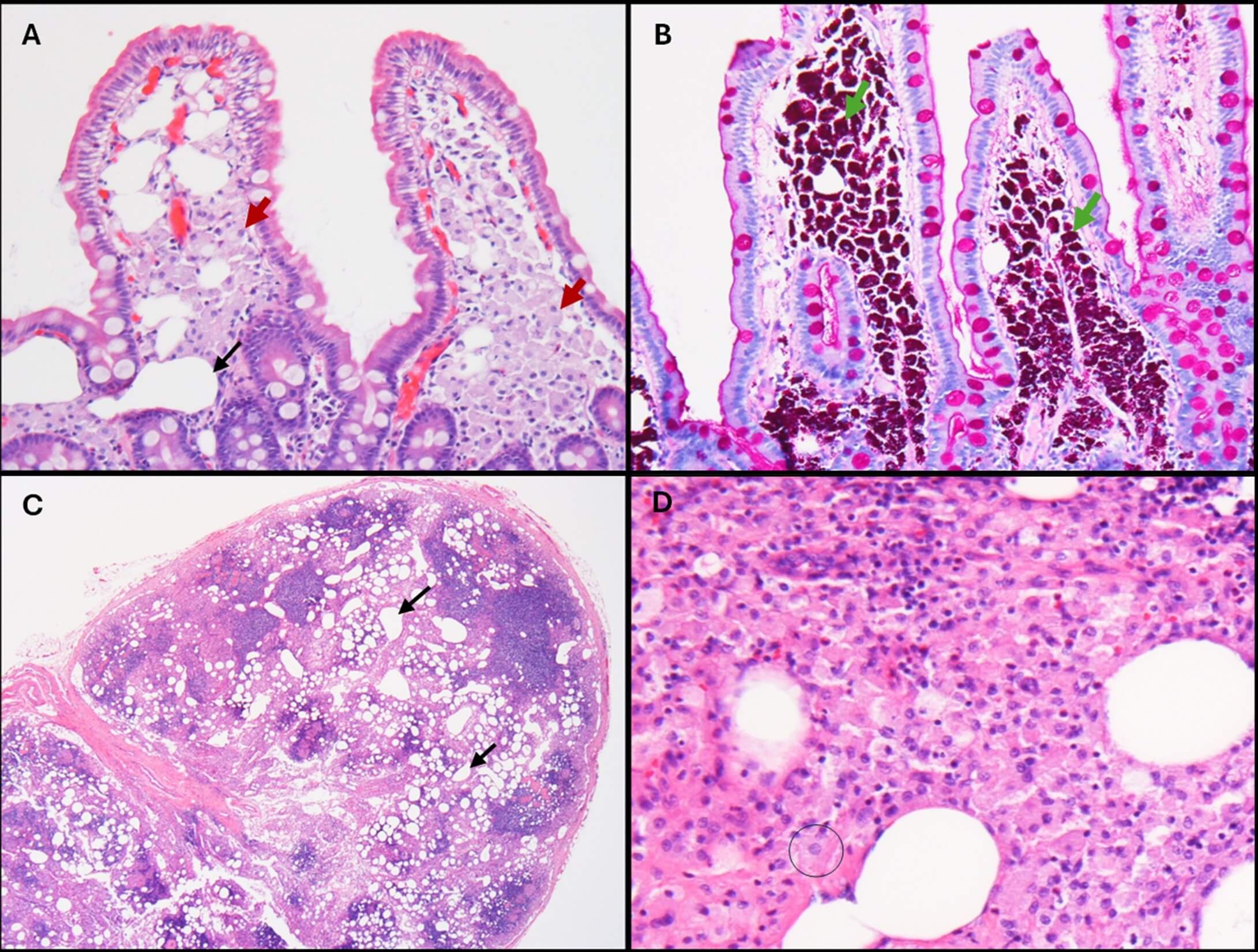
Figure: Figure 2. (A) High-power view of a duodenal biopsy showing lamina propria expanded by macrophages with abundant pink, “foamy” cytoplasm (red arrows). Clear spaces represent dilated lymphatic channels (black arrow). (B) High-power view of the duodenal biopsy with periodic acid–Schiff (PAS) stain. Lamina propria macrophages demonstrate strong PAS positivity (green arrows). (C) Low-power view of a mesenteric lymph node. Dilated lymphatic spaces (black arrows) are seen, with intervening pink areas representing macrophage accumulation. (D) High-power view of the lymph node demonstrating macrophages morphologically similar to those in the duodenal biopsy (black circle)
Disclosures: Samantha Lujan indicated no relevant financial relationships. Daniel Ellis indicated no relevant financial relationships. Diane Nguyen indicated no relevant financial relationships. Jonathan Baker indicated no relevant financial relationships.
Samantha Lujan, MD1, Daniel Ellis, MD2, Diane Nguyen, MD2, Jonathan Baker, MD3. P3466 - Whipple’s Disease Presenting With Peritoneal Nodularity and Pleural Effusion Mimicking Carcinomatosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")