Michael Cymbal, DO1, Renan Prado, MD1, Arjun Chatterjee, MD2, Diego Ramonfaur, MD1, Carmela Tan, MD1, Brian B. Baggott, MD3 1Cleveland Clinic Foundation, Cleveland, OH; 2Gastroenterology and Hepatology, Cleveland Clinic, Cleveland, OH; 3Digestive Disease and Surgery Institute, Cleveland Clinic, Cleveland, OH Introduction: Whipple's disease is a chronic, systemic infection caused by the actinobacterium Tropheryma whipplei. It often presents initially with arthralgia or polyarthralgia, which may precede gastrointestinal symptoms such as diarrhea by months or even years. Its low prevalence and exclusion from standard infectious stool screening panels often preclude timely diagnosis. The diagnosis is histopathological, with small bowel biopsy revealing periodic acid–Shiff (PAS)-positive macrophages in the lamina propria, often accompanied by villous atrophy and foamy macrophage infiltration.
Case Description/
Methods: A 65-year-old man with a history of alcohol and tobacco use disorder presented with exertional shortness of breath, polyarthralgia involving the bilateral wrists, feet, and ankles, unintentional 30-pound weight loss, and intractable watery diarrhea over the last year. Laboratory evaluation revealed mildly elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), with negative infectious workup and autoimmune serologies. Cardiovascular workup showed mitral valve disease with moderate stenosis and severe regurgitation, and 90% right coronary artery stenosis. He was diagnosed with rheumatic fever and underwent mitral valve replacement and CABG.
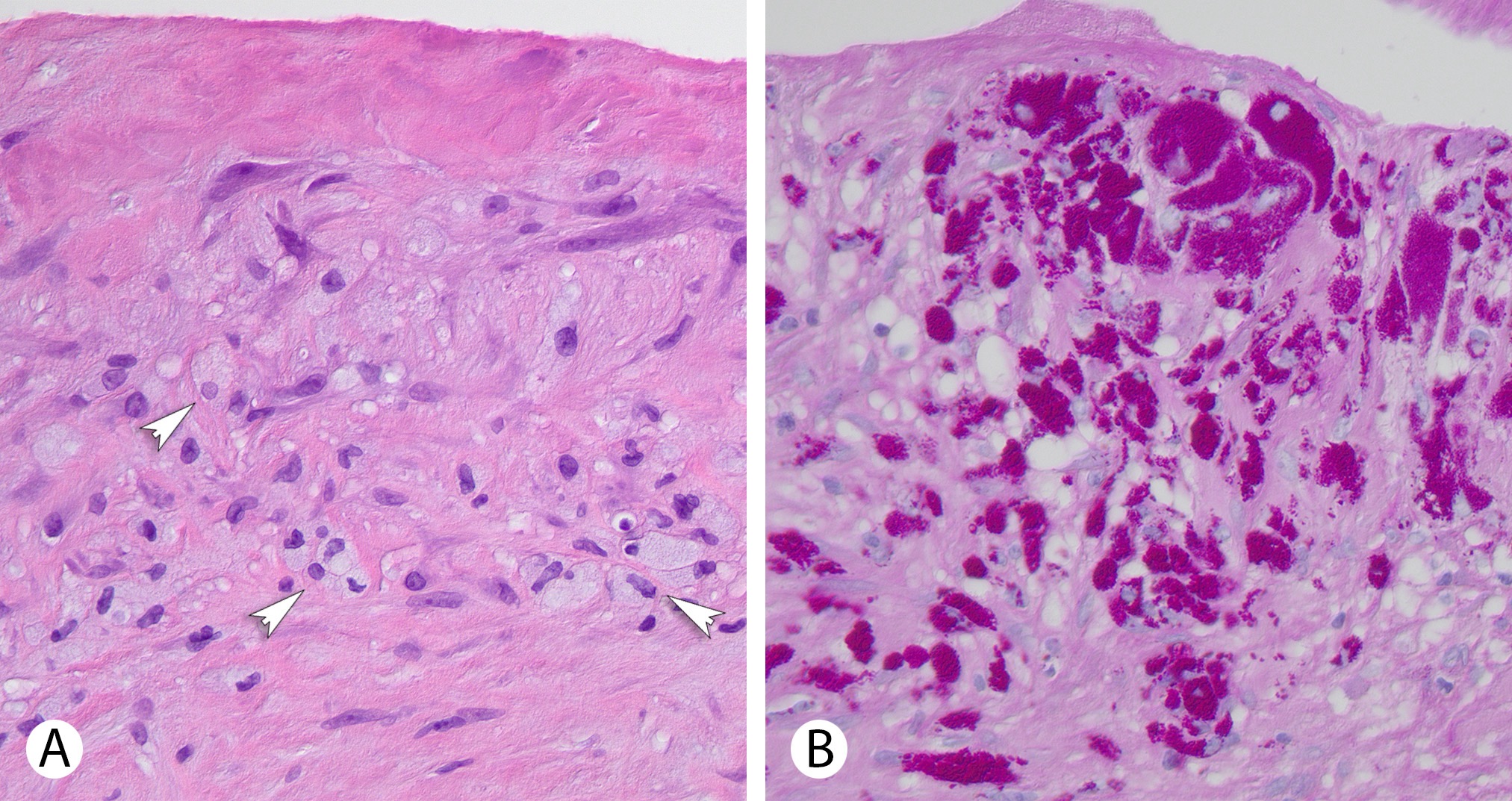
Histopathological examination of the excised mitral valve revealed focal clusters of foamy histiocytes (Figure 1A). Periodic acid–Schiff (PAS) staining demonstrated numerous PAS-positive organisms within histiocytes (Figure 1B), consistent with infective endocarditis due to Tropheryma whipplei. The patient received a four-week course of intravenous ceftriaxone, followed by a two-year course of oral trimethoprim-sulfamethoxazole, resulting in clinical remission of the arthralgia, diarrhea, and weight loss. The patient to date remains on oral antibiotics but has refused endoscopic evaluation to assess for intestinal involvement of Whipple disease. Discussion: This case highlights the stealthy course that Whipple’s disease can take, often mimicking other conditions. This patient had a typical course, diagnosed through an atypical route. Clinical suspicion for Whipple disease must remain high in patients with polyarthralgia and diarrhea with otherwise negative workup. Furthermore, it underscores the importance of timely endoscopic evaluation in patients presenting with unintentional weight loss and altered bowel habits.
Figure: Figure 1A-B: A Histologic section of the mitral valve shows clusters of foamy histiocytes (arrows) in the valve stroma without neutrophils or obvious vegetations (hematoxylin-eosin, 400x). B Periodic acid-Schiff stain highlights numerous histiocytes with PAS-positive organisms
Disclosures: Michael Cymbal indicated no relevant financial relationships. Renan Prado indicated no relevant financial relationships. Arjun Chatterjee indicated no relevant financial relationships. Diego Ramonfaur indicated no relevant financial relationships. Carmela Tan indicated no relevant financial relationships. Brian Baggott indicated no relevant financial relationships.
Michael Cymbal, DO1, Renan Prado, MD1, Arjun Chatterjee, MD2, Diego Ramonfaur, MD1, Carmela Tan, MD1, Brian B. Baggott, MD3. P3462 - Whipple’s Disease Mimicking Rheumatic Fever in a 65-Year-Old Man, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.