University of Arizona College of Medicine, Phoenix VA Medical Center Phoenix, AZ
Award: ACG Presidential Poster Award
Leith Ghani, DO1, Diwanshu Soni, DO2, Yasmin Alishahi, MD1 1University of Arizona College of Medicine, Phoenix VA Medical Center, Phoenix, AZ; 2University of Arizona College of Medicine, Phoenix, Phoenix, AZ Introduction: Coccidioidomycosis is a fungal infection caused by inhalation of Coccidioides spores, endemic to the southwestern U.S. Though typically self-limited, it can disseminate in immunosuppressed individuals. TNF is essential for granuloma formation and pathogen control, making its inhibition a key risk factor for opportunistic infections. Ulcerative colitis (UC) often requires anti-TNF therapy to maintain remission. This case illustrates the complex management of UC in regions endemic for Coccidioides.
Case Description/
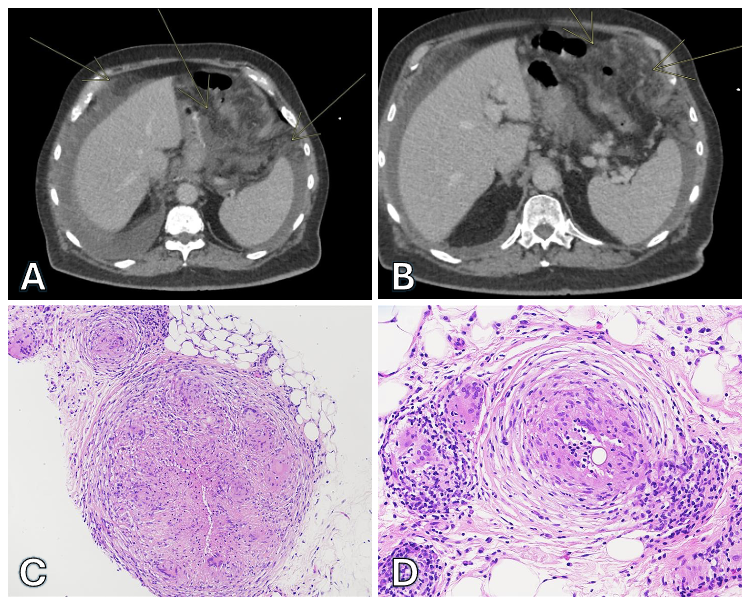
Methods: A 72-year-old male with a 24-year history of UC, maintained in clinical remission with adalimumab, presented with a non-productive cough following a road trip. Chest computed tomography angiography (CTA) revealed a multisegmental pulmonary embolism, right lower lobe pleural effusion, and patchy airspace opacities. Abdominal CTA demonstrated small-to-moderate abdominopelvic ascites, diffuse mesenteric edema, and subsolid nodularity along the omentum and peritoneal surfaces (Figure 1: A and B).
Thoracentesis identified an exudative pleural effusion with negative bacterial and fungal cultures. Coccidioidomycosis serology was positive with a titer of 1:64. Paracentesis revealed an exudative etiology with a serum ascites albumin gradient of 0.4 g/dL. A biopsy of the right upper omentum was performed, showing granulomatous inflammation and fungal organisms consistent with Coccidioides species (Figure 1: C and D). The patient was initiated on fluconazole 400 mg daily and adalimumab was held. Discussion: This case highlights the delicate balance between immunosuppression and infection risk. Anti-TNF agents like adalimumab, while effective in UC, impair the immune system’s ability to contain fungal infections such as Coccidioides. A meta-analysis in IBD showed anti-TNF therapy doubles the risk of opportunistic infections.1 TNF’s role in granuloma formation is crucial for localizing and containing fungal infections, highlighting why the discontinuation of adalimumab was essential in this case to restore effective immune responses. Tissue biopsy confirmed disseminated coccidioidomycosis and guided antifungal treatment with fluconazole which led to clinical improvement. However, holding immunosuppression threatens keeping UC under control. This underscores the need for a multidisciplinary approach, including ID and GI input. Strategies like antifungal prophylaxis, biomarker monitoring, and geography-informed treatment may reduce risk while preserving disease control.
Figure: Figure 1. A and B: Abdominal CTA demonstrated small-to-moderate abdominopelvic ascites, diffuse mesenteric edema, and subsolid nodularity along the omentum and peritoneal surfaces. C and D: H&E stain from the biopsy of the right upper omentum showing granulomatous inflammation and fungal organisms consistent with Coccidioides species.
Disclosures: Leith Ghani indicated no relevant financial relationships. Diwanshu Soni indicated no relevant financial relationships. Yasmin Alishahi indicated no relevant financial relationships.
Leith Ghani, DO1, Diwanshu Soni, DO2, Yasmin Alishahi, MD1. P3386 - Omental Coccidioidomycosis in an Ulcerative Colitis Patient on Immunosuppressive Therapy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.



 photo")