Monday Poster Session
Category: IBD
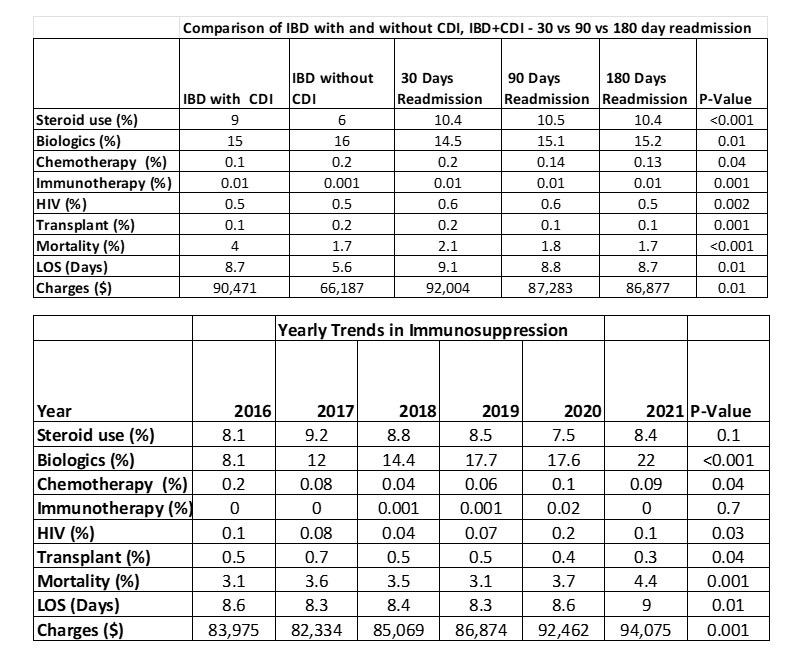
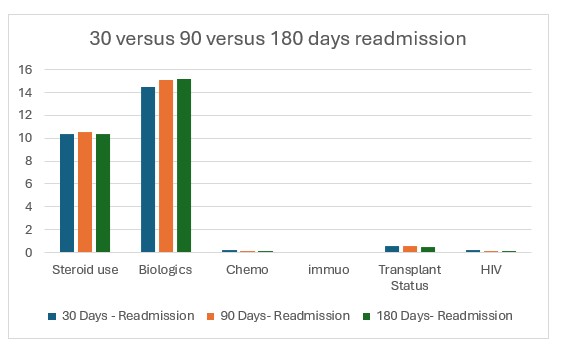
Impact of Immunosuppression on Recurrence of <i>Clostridioides difficile</i> Infection in Inflammatory Bowel Disease
 photo")
Silpa Choday, MD (she/her/hers)
Creighton University School of Medicine
Phoenix, AZ