P3192 - Effects of Subcutaneous Guselkumab Induction and Maintenance on Histologic Outcomes in Patients With Moderately to Severely Active Crohn’s Disease in GRAVITI, a Phase 3 Double-Blind, Placebo-Controlled, Treat-Through Study
Dr. Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA New York, NY
Award: ACG Presidential Poster Award
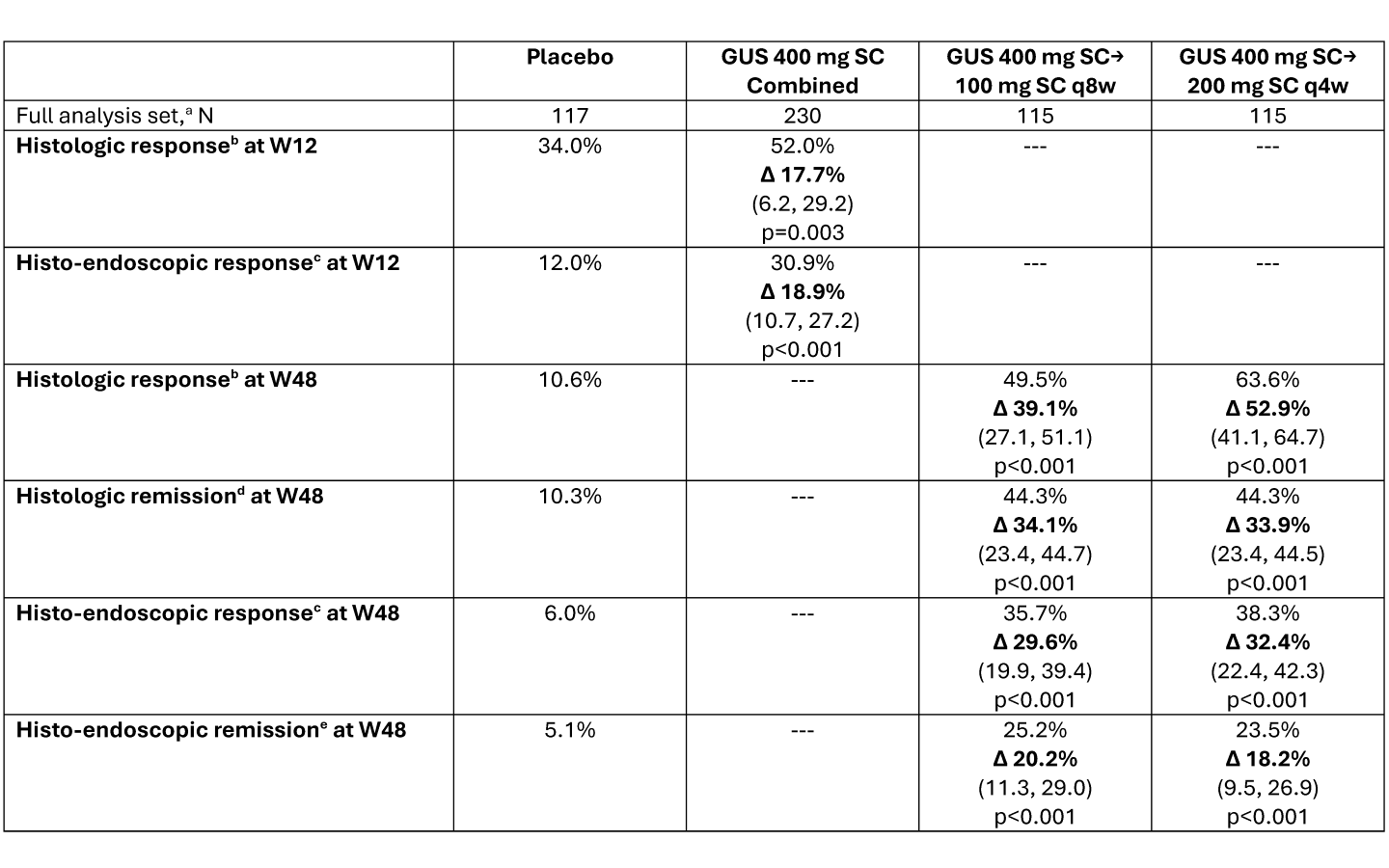
Geert R. D’Haens, MD, PhD1, Ailsa Hart, BA, BMBCh, PhD2, Remo Panaccione, MD3, Flavio Steinwurz, MD, MACG4, Qian Cao, MD, PhD5, Mobolaji Olurinde, MD, PhD6, Leonardo Salese, MD6, Patrick Branigan, BS6, Wilbert van Duijnhoven, MSc7, Nat A. Terry, MD, PhD6, Silvio Danese, MD, PhD8, Tadakazu Hisamatsu, MD, PhD9, Bruce E. Sands, MD, MS, FACG10 1Department of Gastroenterology, Amsterdam University Medical Center, Amsterdam, Noord-Holland, Netherlands; 2London North-West University Healthcare NHS Trust, London, England, United Kingdom; 3Inflammatory Bowel Disease Unit, Division of Gastroenterology and Hepatology, Department of Medicine, University of Calgary, Calgary, AB, Canada, Calgary, AB, Canada; 4Hospital Israelita Albert Einstein, São Paulo, Sao Paulo, Brazil; 5Sir Run Run Shaw Hospital Affiliated with School of Medicine, Zhejiang University, Hangzhou, Zhejiang, China; 6Johnson & Johnson, Spring House, PA; 7Johnson & Johnson, Antwerp, Antwerpen, Belgium; 8Gastroenterology and Endoscopy, IRCCS Ospedale San Raffaele and University Vita-Salute San Raffaele, Milan, Lombardia, Italy; 9Department of Gastroenterology and Hepatology, Kyorin University School of Medicine, Tokyo, Tokyo, Japan; 10Dr. Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA, New York, NY Introduction: Guselkumab (GUS) is a dual-acting IL-23p19 subunit inhibitor that was efficacious in double-blind, placebo-controlled, treat-through trials in participants (pts) with moderately to severely active Crohn’s disease (CD) using IV induction and SC maintenance (GALAXI 2 & 3) or SC induction and maintenance (GRAVITI). Assessment of histologic disease activity is becoming increasingly important as a measure of treatment efficacy. Here we report histologic outcomes at Weeks (W) 12 & 48 from GRAVITI. Methods: Pts were randomized 1:1:1 to GUS 400mg SC q4w→200mg SC q4w, GUS 400mg SC q4w→100mg SC q8w, or PBO. Biopsies were obtained from the most affected area (or if no disease activity present, normal-appearing mucosa) in 5 segments: terminal ileum, ascending colon, transverse colon, descending colon, and rectum. Histologic response, histologic remission, and the composite endpoints of histo-endoscopic response and histo-endoscopic remission were evaluated using Robarts Histopathology Index (RHI), Global Histologic Activity Score (GHAS), and Geboes scoring. Histologic response was assessed in pts with baseline histologic disease; histologic remission, histo-endoscopic response, and histo-endoscopic remission were assessed in the full analysis set (definitions in table legend). Pts who met rescue criteria at W16 were considered non-responders at W48. Histologic endpoints in GRAVITI were exploratory and not controlled for multiple comparisons; p-values are nominal. Results: Of the 347 pts in the full analysis set, 273 (78.7%) had baseline histologic disease per RHI score. SC induction with GUS (400mg SC at W0, W4, & W8) resulted in greater rates of histologic response, histologic remission, histo-endoscopic response, and histo-endoscopic remission compared to placebo at W12 (Table). At W48, greater proportions of pts receiving GUS 100mg SC q8w or GUS 200mg SC q4w maintenance also achieved histologic response, histologic remission, histo-endoscopic response, and histo-endoscopic remission compared to PBO. Comparable outcomes were observed using GHAS or Geboes scoring criteria. Discussion: Compared to PBO, pts with moderately to severely active CD receiving SC induction and maintenance treatment with GUS achieved greater rates of histologic response, histologic remission, histo-endoscopic response, and histo-endoscopic remission through W48. These results support the use of histologic and composite histologic and endoscopic endpoints as a measure of CD activity, and the efficacy of SC guselkumab in CD.
Figure: Data presented as percentage of participants attaining the endpoint, with adjusted treatment difference (Δ), (95% confidence interval), and nominal p-value versus placebo. Adjusted treatment differences, 95% CIs, and p-values were based on the common risk difference by use of Mantel-Haenszel stratum weights and the Sato variance estimator, using stratification factors of baseline CDAI score (≤300 or >300), baseline SES-CD (≤12 or >12), and prior history of inadequate response or intolerance to biologics (Yes or No). Participants who had a CD-related surgery (with the exception of minor procedures such as drainage of a superficial abscess or seton placement, etc.), had a prohibited change in CD medication, discontinued study intervention for any reason (other than COVID-19 related reasons [excluding COVID-19 infection] or regional crisis), or met rescue criteria (only applicable after Week 16) were considered not to have met the endpoint at the designated timepoint. Participants who discontinued study intervention due to COVID-19 related reasons (excluding COVID-19 infection) or regional crisis had their observed data used, if available. After accounting for the aforementioned data handling rules, participants who were missing data pertaining to an endpoint at a designated timepoint were considered not to have achieved the endpoint. DEFINITIONS: a. Full analysis set: all randomized participants who received ≥1 dose of study medication. b. Histologic response: ≥50% reduction in RHI score from baseline or a score ≤ 3 with sub-scores of lamina propria neutrophils and neutrophils in epithelium must be equal to 0, with no ulcers or erosions. Assessed in participants in the full analysis set with baseline histologic disease, defined as RHI score > 0 for any of Items 2-4 of RHI (lamina propria neutrophils, neutrophils in epithelium, or erosions or ulcerations); N = placebo (94), GUS 400mg SC Combined (179), GUS 400mg SC→100mg SC q8w (91), GUS 400mg SC→200mg SC q4w (88). c. Histo-endoscopic response: ≥50% reduction in RHI score from baseline or a score ≤ 3 with sub-scores of lamina propria neutrophils and neutrophils in epithelium must be equal to 0, with no ulcers or erosions AND ≥50% improvement from baseline in SES-CD or SES-CD ≤ 2. Assessed in the full analysis set. d. Histologic remission: RHI score ≤ 3 with sub-scores of lamina propria neutrophils, neutrophils in the epithelium and erosions or ulcerations equal to 0. Assessed in the full analysis set. e. Histo-endoscopic remission: RHI score ≤ 3 with sub-scores of lamina propria neutrophils, neutrophils in the epithelium and erosions or ulcerations equal to 0 AND SES-CD ≤ 4 and at least a 2-point reduction from baseline and no subscore greater than 1 in any individual component. Assessed in the full analysis set.