P3162 - Gastroenterologist Follow-Up Is Associated With Reduced Readmission Compared to Primary Care After Hospitalization for Severe Ulcerative Colitis
Ola Selnes, BSc1, Justin Zhuo, MD2, Sarah Streett, MD1, Grant Barber, MD, MS1 1Stanford Health Care, Stanford, CA; 2Robert Wood Johnson Medical School, Rutgers University, New Brunswick, NJ Introduction: Patients hospitalized for severe ulcerative colitis (UC) flares are at high risk of readmission, yet guidelines offer limited direction for post-discharge care. Prior studies suggest timely outpatient follow-up with a gastroenterology (GI) specialist may reduce readmission risk, but the impact of provider type remains unclear. We aimed to determine whether post-discharge follow-up with a primary care provider (PCP) influences readmission risk. Methods: We conducted a retrospective cohort study of patients hospitalized for UC flare at Stanford University Hospital between 2010 and 2021. The primary outcome was time to a GI-related readmission. The primary exposure was provider type at first follow-up visit (GI vs PCP vs no follow-up), modeled as a time-dependent covariate in Cox proportional hazards regression. Models were adjusted for age, sex, and albumin at admission. Kaplan-Meier and log-rank tests compared cumulative readmission risk between PCP follow-up and no follow-up. Results: Of the 223 patients included for analysis, 156 (70.0%) had follow-up with a GI specialist, 28 (12.3%) had PCP follow-up, and 39 (17.4%) had no follow-up during the study period. Median time to follow-up was shorter in the PCP group (5 days, IQR 6 days) than in the GI specialist group (10 days, IQR 14 days). PCP follow-up was not associated with reduced readmission compared to no follow-up (adjusted HR 1.40; 95%-CI, 0.63-3.15; p=0.41). Follow-up with a GI specialist was associated with a significantly lower readmission risk (adjusted HR 0.46; 95%-CI, 0.24-0.87; p=0.016). Discussion: Our results highlight the importance of provider type in post-discharge care after hospitalization for severe UC. Despite earlier follow-up, PCP evaluation did not reduce readmissions, while follow-up with a GI specialist was significantly associated with reduced readmission rates. This suggests that GI-specific care in the post-discharge phase is important for recognizing early relapse, optimizing therapies, and preventing readmissions. Thus, ensuring access to GI should be prioritized in care pathways for post-discharge UC management. To further elucidate this, future studies should evaluate whether follow-up with GI-specific advanced practice providers confers a similar reduction of readmissions.
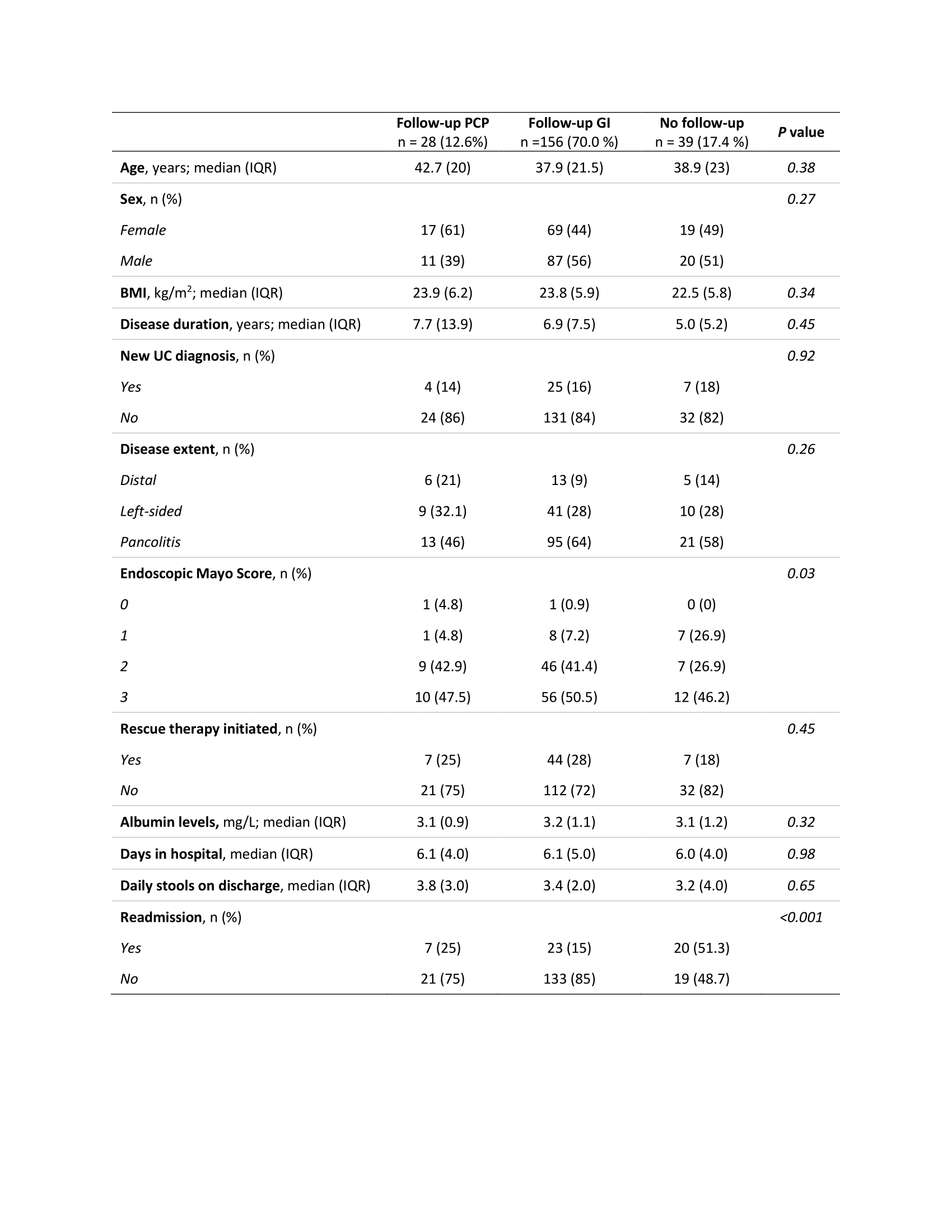
Figure: Table 1. Characteristics of study participants stratified by follow-up with PCP, GI specialist, or no follow-up.
Abbreviations: BMI, body mass index; UC, ulcerative colitis. P values are generated by chi-squared-test and Fisher’s exact test (if <5 observation in ≥1 cell for a variable) for categorical variables, and ANOVA for continuous variables.
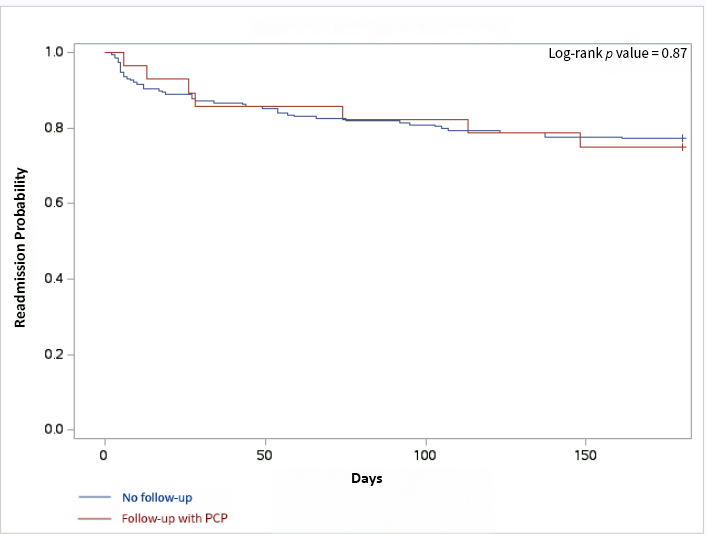
Figure: Figure 1. Kaplan-Meyer curve. Readmission probability following 180 days after discharge with PCP follow-up versus no follow-up.
Disclosures: Ola Selnes indicated no relevant financial relationships. Justin Zhuo indicated no relevant financial relationships. Sarah Streett: Bristol Myers Squibb – Advisory Committee/Board Member. Direct Biologics – Advisory Committee/Board Member. gilead – Consultant. janssen – Advisory Committee/Board Member. Takeda – Advisory Committee/Board Member. Grant Barber indicated no relevant financial relationships.
Ola Selnes, BSc1, Justin Zhuo, MD2, Sarah Streett, MD1, Grant Barber, MD, MS1. P3162 - Gastroenterologist Follow-Up Is Associated With Reduced Readmission Compared to Primary Care After Hospitalization for Severe Ulcerative Colitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.