Alexander Zhu, DO1, Meghan Cloutier, MD1, Edward Tamale, MD1, Jenna Dawson, MD1, Anand Bhagat, DO2, Mark Michael, MD1, Thomas Mahl, MD1 1University at Buffalo, Buffalo, NY; 2Baptist Health Bethesda Hospital, Boynton Beach, FL Introduction: Upper gastrointestinal bleeding (UGIB) is a common complication of peptic ulcer disease, most often due to erosion into the gastroduodenal artery (GDA). In rare cases, a duodenal ulcer can erode into the gallbladder, forming a cholecystoduodenal fistula (CDF) that exposes the cystic artery to injury and hemorrhage. This exceptionally uncommon complication has historically been managed surgically. We present a case of ulcer-related CDF complicated by cystic artery hemorrhage, successfully managed nonoperatively.
Case Description/
Methods: A 62-year-old male with history of H. pylori infection and GDA embolization for UGIB presented with weakness, melena, and hematochezia. He was admitted for hemorrhagic shock with hemoglobin of 3.6 g/dL. CT angiography (CTA) showed no extravasation but revealed a lobulated, thickened gallbladder wall and pericholecystic fluid concerning for localized perforation. Repeat CTA showed active extravasation near the second portion of the duodenum, adjacent gas and fluid, and lobulated partially nonenhancing gallbladder suspicious for rupture or fistulization. Angiography confirmed extravasation from a branch of the cystic artery, which was treated with coil embolization. Post-procedural ultrasound showed intraluminal gallbladder gas and spontaneous decompression into the duodenum. Follow-up CT with oral and IV contrast showed contrast tracking through the gallbladder wall toward the duodenum, further supporting diagnosis of CDF. Cholecystostomy was considered but deferred due to clinical stability and evidence of spontaneous gallbladder decompression. The patient was managed with supportive care and broad-spectrum antibiotics, later transitioned to H. pylori eradication therapy following a positive stool antigen test. Discussion: Ulcer-related CDF involving the cystic artery is a rare and diagnostically challenging cause of UGIB. Most biliary-enteric fistulas arise from gallstones, while duodenal ulcer erosion into the gallbladder causing cystic artery hemorrhage is exceptionally rare and typically requires surgery. Diagnosis may be challenging due to nonspecific imaging findings. In this case, angiography was critical in localizing and treating the bleed with coil embolization. While post-embolization gallbladder infarction is a potential complication, collateral blood supply often mitigates this risk. This case demonstrates the potential for nonoperative management with angiographic embolization in select patients with ulcer-related cystic artery hemorrhage.
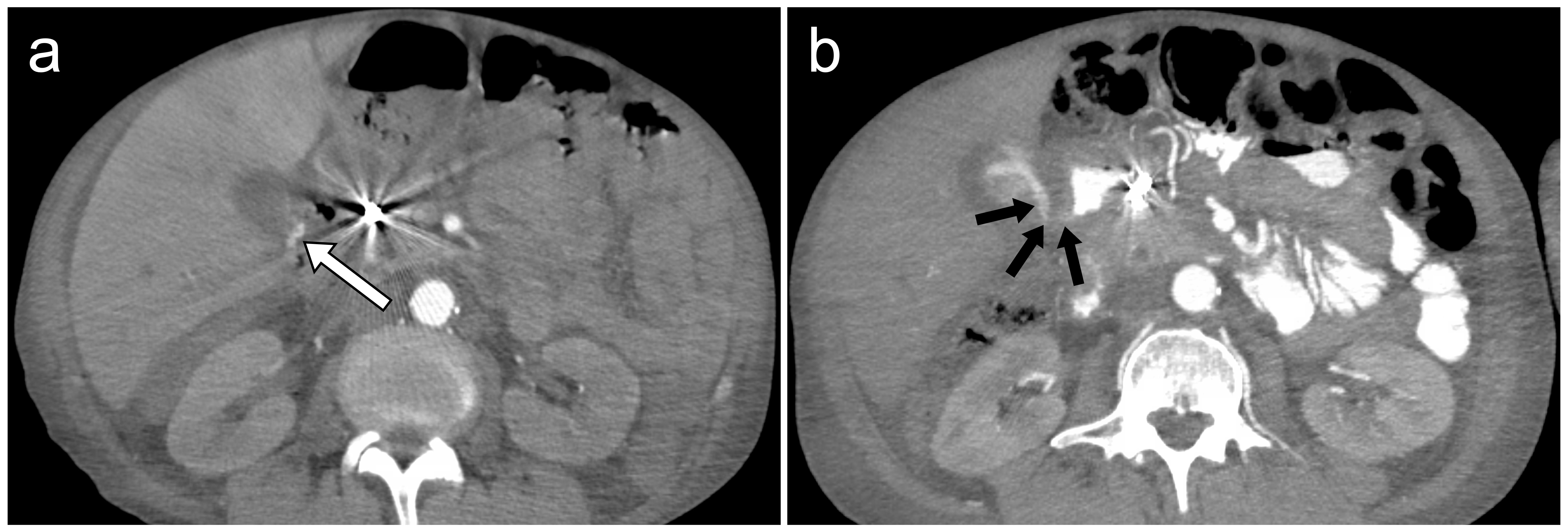
Figure: Figure 1. (a) CT angiography showing active extravasation (white arrow) adjacent to the second portion of the duodenum with adjacent gas and fluid. (b) Post-embolization CT with oral and IV contrast showing contrast tracking through the gallbladder wall (black arrows) toward the duodenum, consistent with cholecystoduodenal fistula.
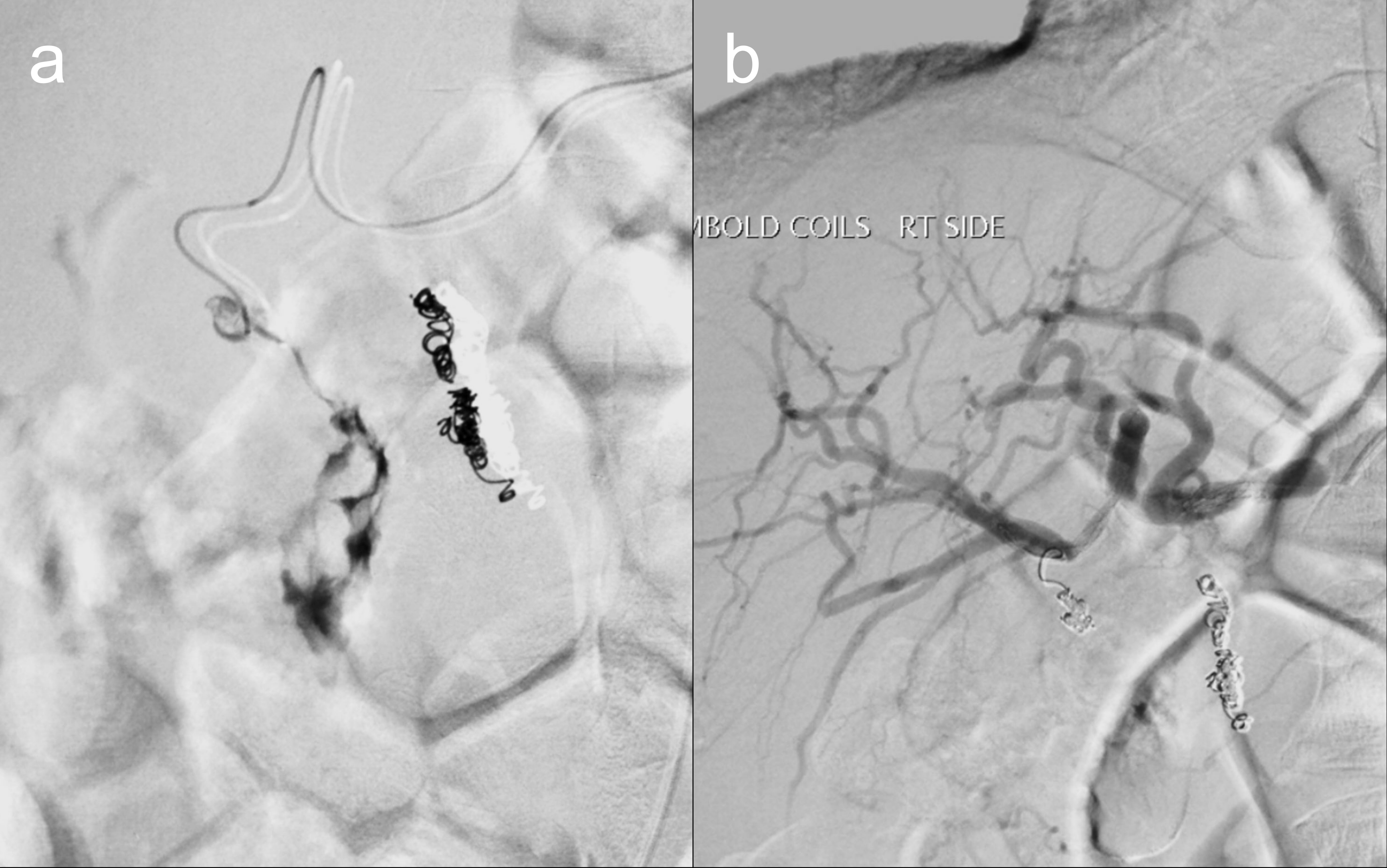
Figure: Figure 2. (a) Angiography demonstrating active extravasation from a branch of the cystic artery. (b) Post-embolization angiogram showing successful coil embolization with no residual contrast extravasation.
Disclosures: Alexander Zhu indicated no relevant financial relationships. Meghan Cloutier indicated no relevant financial relationships. Edward Tamale indicated no relevant financial relationships. Jenna Dawson indicated no relevant financial relationships. Anand Bhagat indicated no relevant financial relationships. Mark Michael indicated no relevant financial relationships. Thomas Mahl indicated no relevant financial relationships.
Alexander Zhu, DO1, Meghan Cloutier, MD1, Edward Tamale, MD1, Jenna Dawson, MD1, Anand Bhagat, DO2, Mark Michael, MD1, Thomas Mahl, MD1. P3105 - Ulcer-Related Cystic Artery Hemorrhage and Cholecystoduodena Fistulal: A Rare Case Managed Nonoperatively, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.