University of Central Florida, HCA Healthcare GME Pensacola, FL
Priya Kumari Maheshwari, MD1, Shahroz Fatima, MD2, John Paul Nsubuga, MD3, Eman Kazi, MD3, Arlen Brickman, MD3, Amer B. Malik, MD4, Li Wang, MD3 1University of Central Florida, HCA Healthcare GME, Pensacola, FL; 2Brown University / Rhode Island Hospital, Warwick, RI; 3Brown University / Rhode Island Hospital, Providence, RI; 4Warren Alpert Medical School of Brown University, Providence, RI Introduction: Aortoesophageal fistula (AEF) is a rare, often fatal cause of upper gastrointestinal (GI) bleeding, typically resulting from thoracic aortic aneurysms, malignancy, foreign body ingestion, or prior aortic interventions. It classically presents with a herald bleed followed by catastrophic hemorrhage. While secondary AEFs typically occur near grafts, spontaneous fistulas in remote, non-grafted segments are rare. We present a case of spontaneous AEF five weeks after ascending aortic repair in a location remote from the graft.
Case Description/
Methods: A 64-year-old male with obesity and hypertension presented with chest pain and was diagnosed with an aortic dissection from the thoracic aorta to the iliac arteries. He underwent emergent ascending aortic repair with graft placement with eventual stable discharge. About 5 weeks later, he presented again with chest pain, dyspnea, and melena.
Initial vitals were: temperature 97.6°F, BP 131/72 mmHg, pulse 54 bpm, RR 22, and SpO₂ 98% on room air. Hemoglobin was 7.2 g/dL, down from 9.8 at discharge. Computed Tomography Angiography (CTA) showed a new dissection flap distal to the left subclavian and descending to the left iliac artery with left renal infarction, consistent with a Type B aortic dissection. He was started on intravenous proton pump inhibitors, and melena temporarily resolved.
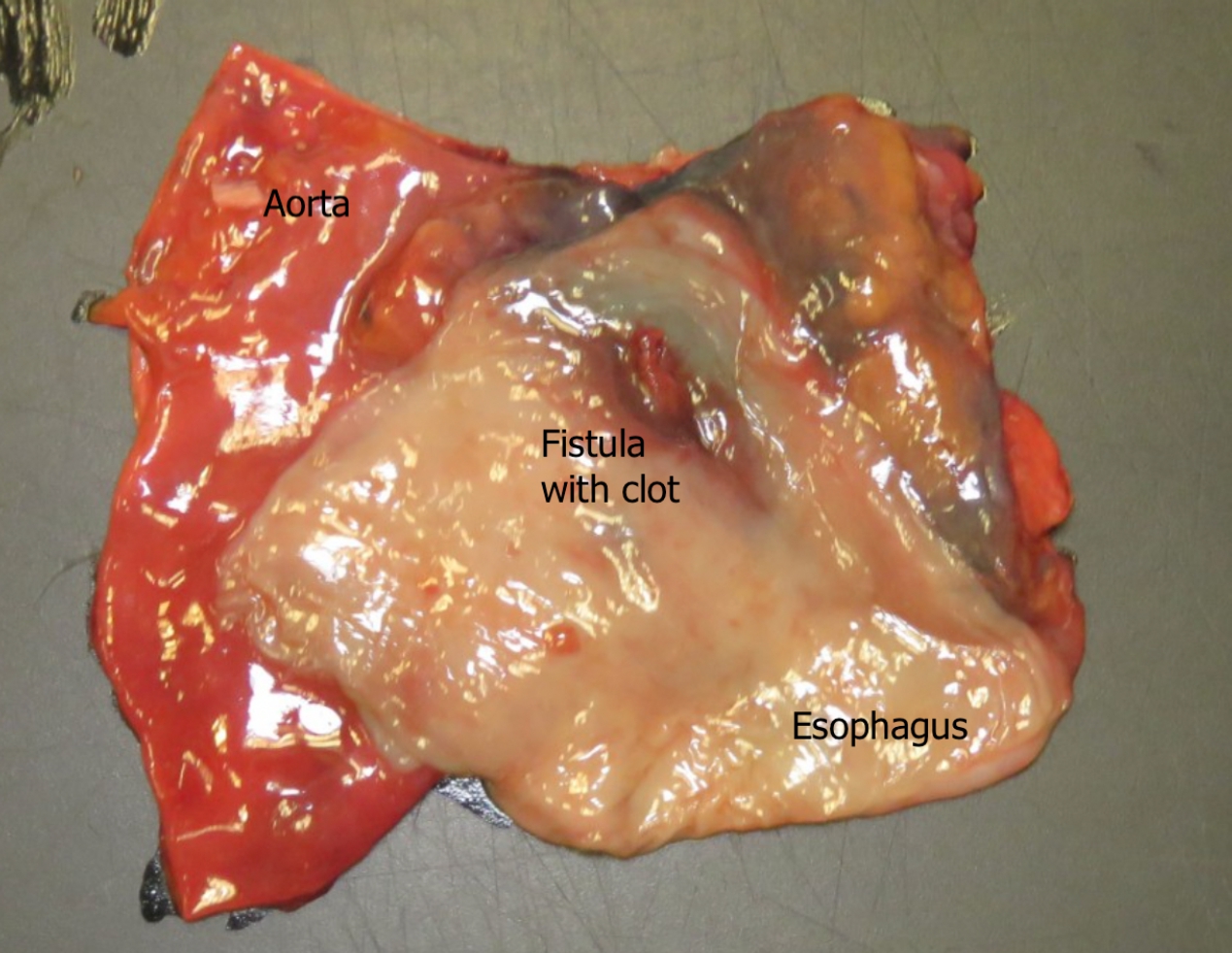
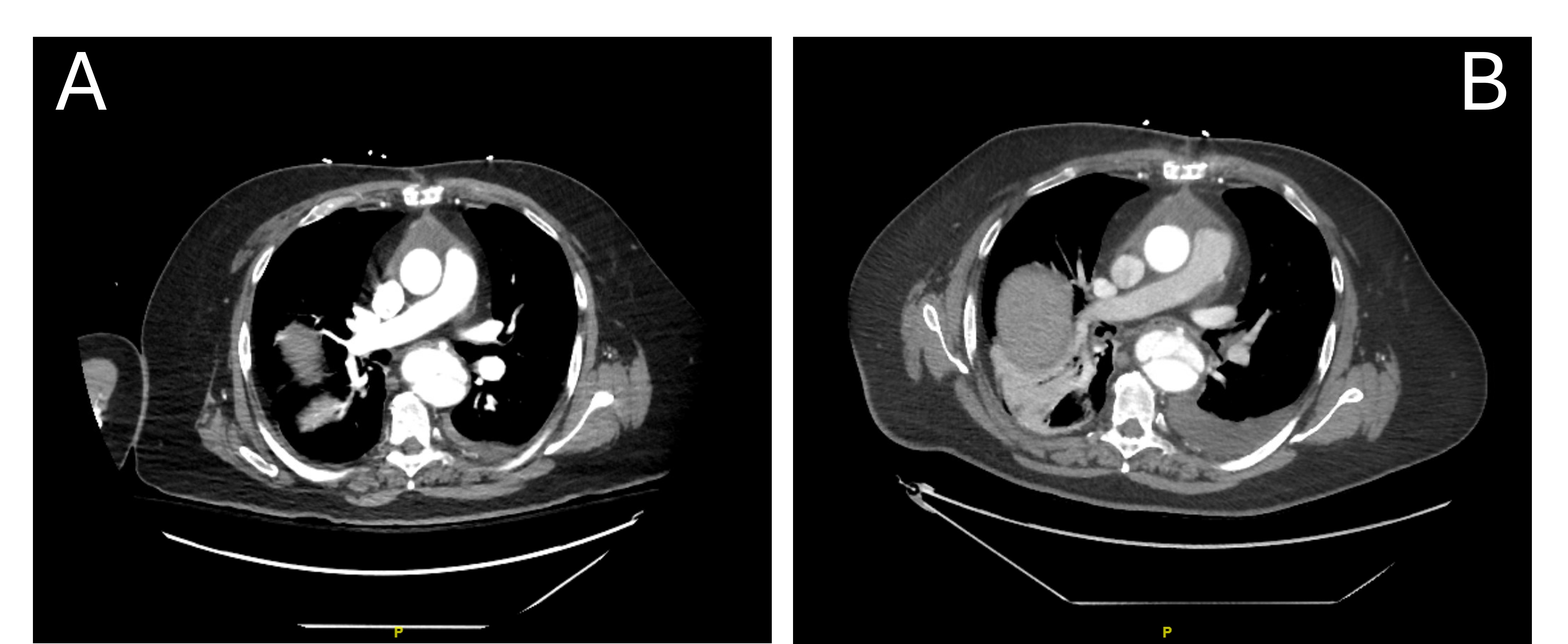
On hospital day five, he developed recurrent melena, hematemesis, and hemodynamic instability. Repeat CTA showed a 7 mm pseudoaneurysm (Figure 1A-B) of the descending thoracic aorta. Despite transfusions and supportive care, he suffered massive hematemesis and cardiac arrest. Emergent endoscopy revealed copious upper GI bleeding without a clear source. The procedure was aborted due to cardiovascular collapse, and the patient died. Autopsy confirmed a spontaneous AEF remote from the graft (Figure 2). Discussion: This case illustrates a rare AEF remote from the graft site in the setting of a Type B aortic dissection. Although prior aortic interventions, such as grafting, are known risk factors, this unusual fistula developed in the context of progressive aortic dissection without direct graft involvement, a rarely reported phenomenon. The rapid progression from herald bleed to exsanguination underscores the fatal nature of AEF and the need for high clinical suspicion in patients with aortic disease and GI bleeding, regardless of graft site.
Figure: Figure 1A–B: Axial CTA images showing a pseudoaneurysm of the descending thoracic aorta, concerning for impending aortoesophageal fistula.
Figure: Figure 2: Gross autopsy specimen showing a spontaneous aortoesophageal fistula with clot, connecting the descending thoracic aorta and esophagus, remote from the prior graft site.
Disclosures: Priya Kumari Maheshwari indicated no relevant financial relationships. Shahroz Fatima indicated no relevant financial relationships. John Paul Nsubuga indicated no relevant financial relationships. Eman Kazi indicated no relevant financial relationships. Arlen Brickman indicated no relevant financial relationships. Amer Malik indicated no relevant financial relationships. Li Wang indicated no relevant financial relationships.
Priya Kumari Maheshwari, MD1, Shahroz Fatima, MD2, John Paul Nsubuga, MD3, Eman Kazi, MD3, Arlen Brickman, MD3, Amer B. Malik, MD4, Li Wang, MD3. P3103 - The Deadly Leak: An Unusual Location of a Post-Repair Aortoesophageal Fistula, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")