Beishi Zheng, MD1, Julio C. Valencia-Manrique, MD1, Oyedotun Babajide, MD1, Gulce Karaca, MD2, Dalia Mahmoud Hassan Elamin, MD2 1NYC Health + Hospitals/Metropolitan, New York, NY; 2NYC Health + Hospitals/Woodhull, Brooklyn, NY Introduction: Gastric varices are typically caused by liver cirrhosis, portal vein thrombosis, or splenic vein thrombosis. Non-cirrhotic, non-portal hypertensive gastric varices are rare. Here, we present a case in which unique vascular anatomy and prior surgical history led to the development of gastric varices.
Case Description/
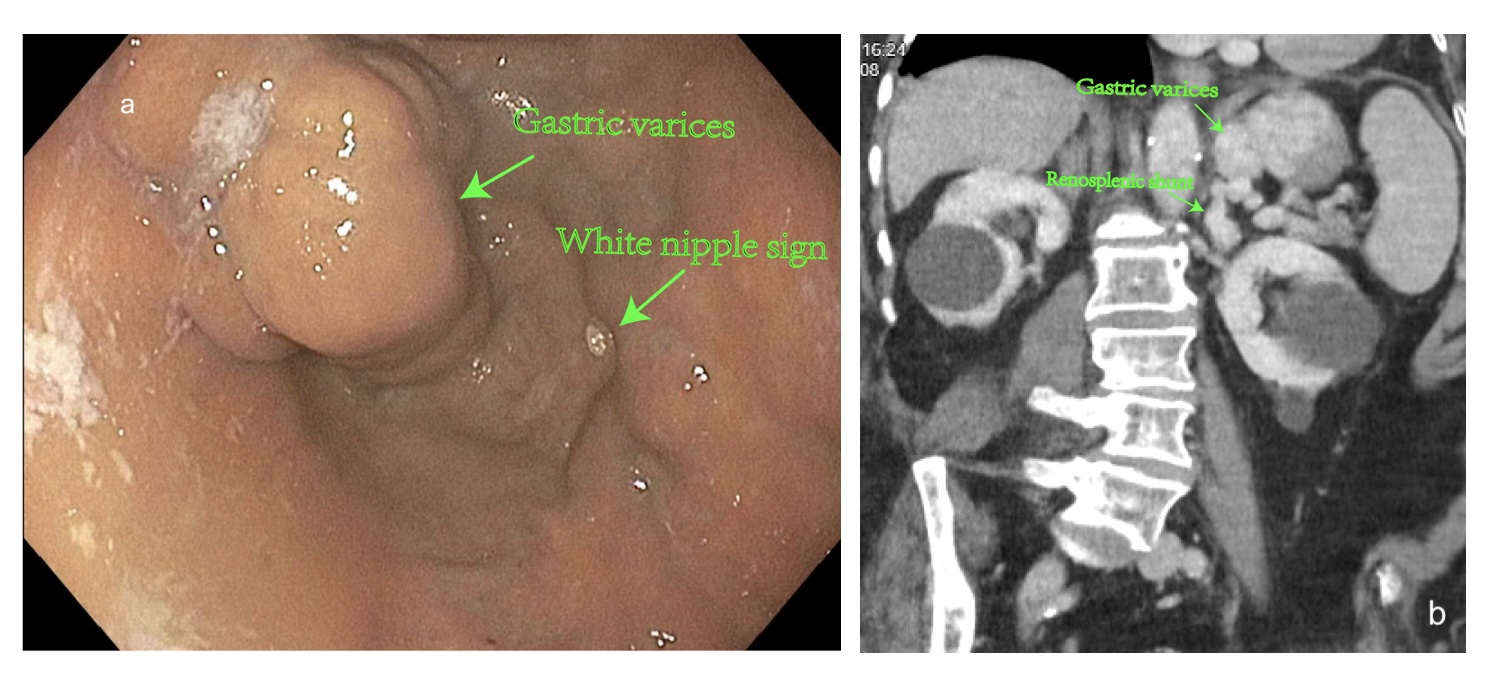
Methods: An 81-year-old female with a past surgical history of total hysterectomy with bilateral salpingo-oophorectomy (BSO) presented to the emergency room with severe anemia and recent episodes of melena. EGD revealed isolated large gastric varices with signs of recent bleeding(pic a). Endoscopic intervention was deferred due to unavailability of coils for eradication of varices and due to lack of active bleeding. A CT angiogram was subsequently performed to evaluate potential interventional radiology options.
Imaging revealed a rare retro-aortic anatomy of the left renal vein, which passed posterior to the aorta rather than in its usual anterior position(Pic c). Additionally, the patient had previously undergone hysterectomy with bilateral oophorectomy, during which the left gonadal vein—a potential collateral pathway—had been ligated(pic d). As a result, the patient developed a rare renosplenic shunt(pic b and pic d), leading to retrograde blood flow into the gastric veins and the formation of varices. Discussion: This case represents a rare cause of non-cirrhotic, non-portal hypertensive gastric varices. It highlights the importance of assessing renal vein anatomy, particularly the presence of a retro-aortic left renal vein, in patients undergoing pelvic surgery such as oophorectomy. Awareness of such vascular variants may help prevent future complications associated with altered venous drainage.
Figure: a. Gastric varices with white nipple sign b. Gastric varices and renosplenic shunt on CT scan.
Figure: c. Retro-aortic anatomy of the left renal vein d. Renosplenic shunt and ligated left gonadal vein.
Disclosures: Beishi Zheng indicated no relevant financial relationships. Julio Valencia-Manrique indicated no relevant financial relationships. Oyedotun Babajide indicated no relevant financial relationships. Gulce Karaca indicated no relevant financial relationships. Dalia Mahmoud Hassan Elamin indicated no relevant financial relationships.
Beishi Zheng, MD1, Julio C. Valencia-Manrique, MD1, Oyedotun Babajide, MD1, Gulce Karaca, MD2, Dalia Mahmoud Hassan Elamin, MD2. P3088 - Non-Cirrhotic Gastric Varices Due to Retro-Aortic Left Renal Vein and Renosplenic Shunt Following Pelvic Surgery: A Rare Vascular Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")