Sheel Patel, DO, Dylan Flaherty, DO, Nana Baah, MD, Endashaw Omer, MD University of Louisville, Louisville, KY Introduction: Gastric variceal bleeding is a serious and potentially fatal consequence of portal hypertension. When endoscopic and pharmacologic measures fail, transjugular intrahepatic portosystemic shunt (TIPS) with coil embolization is a highly effective therapy. While generally safe, rare complications like coil migration can result in gastrointestinal bleeding, perforation, or even cardiac or pulmonary embolization. Migration typically occurs early, within weeks to months. We present a highly unusual case of delayed, asymptomatic coil migration discovered three years post-embolization, with the coil still embedded in the gastric varix and unraveling into the duodenum, highlighting a previously undocumented pattern of migration.
Case Description/
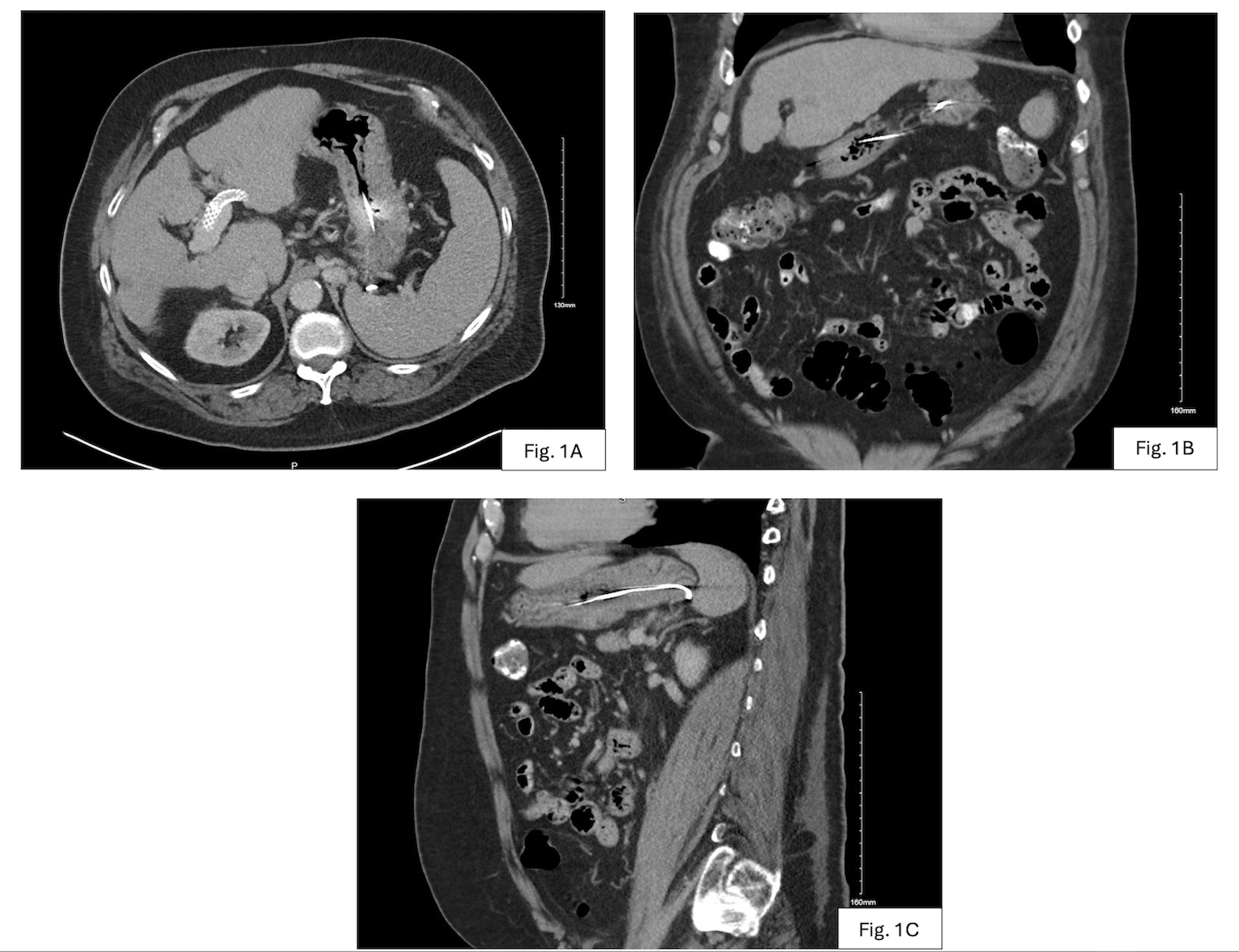
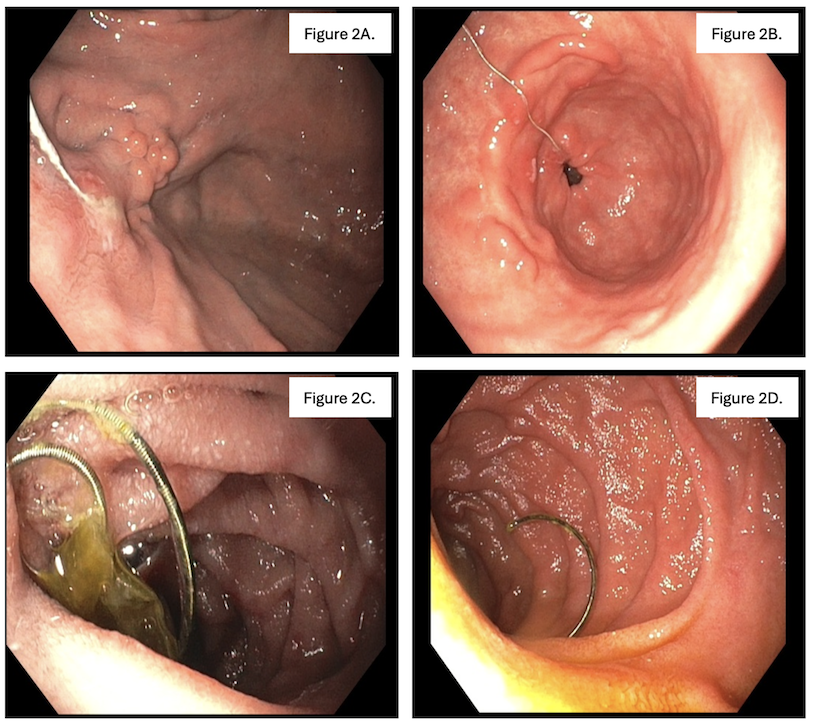
Methods: A 66-year-old man with cirrhosis and prior gastric variceal bleeding underwent TIPS and coil embolization using five coils without adjunctive glue or gelatin. Three years later, he presented with vague abdominal discomfort. CT scan revealed a wire-like metallic density extending from the stomach into the third portion of the duodenum (Fig. 1). EGD confirmed an unraveled coil still anchored within a decompressed gastric varix (GOV2), with distal extension into the duodenum (Fig. 2). There was no evidence of ulceration, erosion, or bleeding. Given the high procedural risk and absence of symptoms, conservative management was selected, and the patient was discharged with monitoring instructions and return precautions. Discussion: This is the first reported case of delayed duodenal coil migration where the coil remained partially embedded in the varix—a unique presentation that expands our understanding of this rare complication. The likely mechanism involved suboptimal packing density and the absence of adhesive agents. Clinicians should be aware that migration can occur silently over extended periods. We recommend structured surveillance with endoscopy or imaging at 6 months and annually thereafter, along with urgent evaluation for any new symptoms. This case underscores the importance of maintaining long-term vigilance after coil embolization, even in the absence of early complications.
Figure: Figure 1: Computed tomography scan (CT) of the abdomen/pelvis showing a thin-metallic object within the duodenum and stomach. Transverse view (1A), Coronal view (1B), and Sagittal view (1C).
Figure: Figure 2: Coil embedded in a previous gastric varix (2A). Coil transversing through the gastric antrum (2B). The coil moves through the small intestine (2C). The distal end of the coil ends in the second portion of the duodenum (2D).
Disclosures: Sheel Patel indicated no relevant financial relationships. Dylan Flaherty indicated no relevant financial relationships. Nana Baah indicated no relevant financial relationships. Endashaw Omer indicated no relevant financial relationships.
Sheel Patel, DO, Dylan Flaherty, DO, Nana Baah, MD, Endashaw Omer, MD. P3020 - Unraveled: Coil Migration After Embolization of Gastric Varices, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.