Sheel Patel, DO, Endashaw Omer, MD University of Louisville, Louisville, KY Introduction: Barrett’s esophagus (BE) is a known precursor to esophageal adenocarcinoma, typically presenting with flat mucosal changes and low-grade dysplasia. However, large polypoid lesions are exceedingly rare and poorly characterized. We present a highly unusual case of BE manifesting as a 25 cm circumferential, friable, polypoid mass with foveolar-type dysplasia, highlighting an underrecognized morphological spectrum of BE and raising new questions in diagnosis and surveillance.
Case Description/
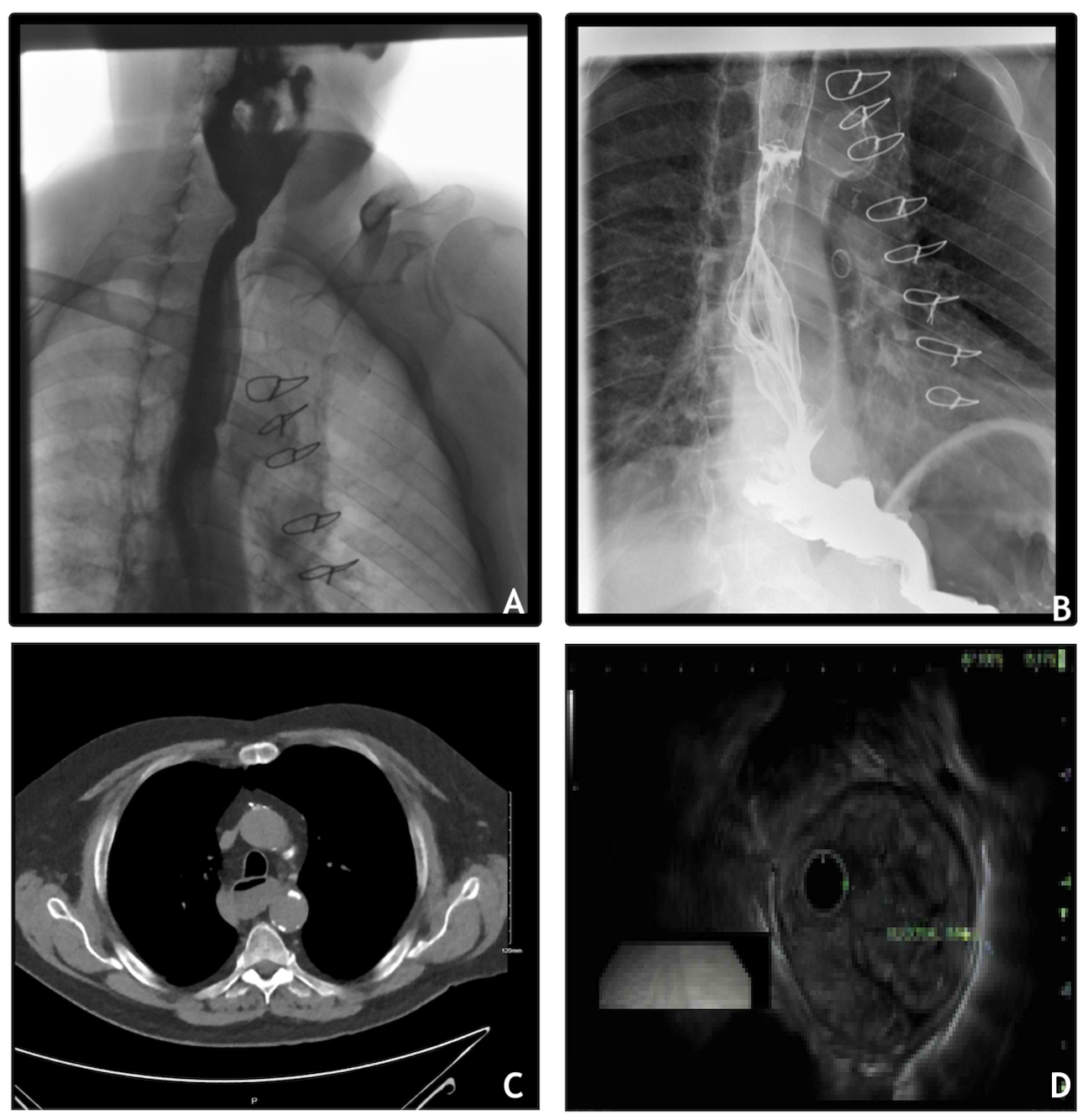
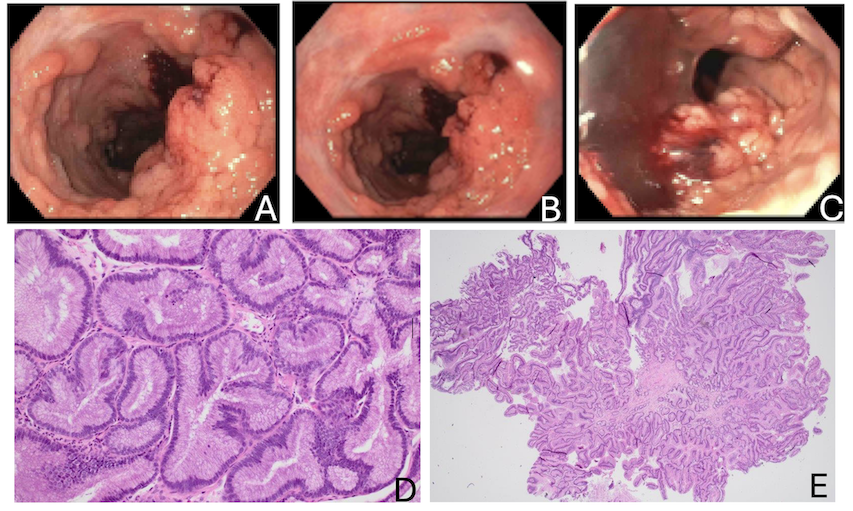
Methods: A 76-year-old man with no prior gastrointestinal workup underwent low-dose chest CT for lung cancer screening, incidentally revealing a distended esophagus and hiatal hernia (Figure 1C). He reported mild dysphagia but denied reflux, weight loss, or NSAID use. Esophagram showed fixed narrowing of the mid-to-distal esophagus and delayed transit (Fig. 1A/B). EGD revealed a 25 cm circumferential, frond-like polypoid mass extending from 20 to 45 cm, involving the entire esophageal circumference (Fig. 2A-C). Biopsies from multiple levels demonstrated papillary glandular epithelium with focal low-grade, foveolar-type dysplasia, but no high-grade dysplasia or carcinoma (Fig. 2D/E). Endoscopic ultrasound showed a thickened mucosal lesion with no submucosal invasion (Fig. 1D). Given the absence of severe symptoms or malignancy, conservative management with surveillance EGDs every six months was recommended. Discussion: This case represents an extraordinarily rare, extensive polypoid manifestation of BE with foveolar-type low-grade dysplasia—a subtype typically seen in gastric mucosa. Its circumferential growth pattern and frond-like morphology mimic neoplasms, complicating diagnosis. The foveolar subtype’s malignant potential remains unclear, but studies suggest an association with molecular instability. In the absence of high-grade dysplasia or invasion, close endoscopic surveillance remains the mainstay of management. This case highlights the diagnostic uncertainty surrounding atypical BE presentations and underscores the importance of thorough histopathological assessment and individualized surveillance plans. These presentations may be underrecognized, and further investigation is warranted to better define their natural history, malignant potential, and evidence-based management strategies.
Figure: Figure 2: A) Upper esophagus B) Mid esophagus C) Distal esophagus D) 200x histology showing nuclei located basally, columnar or pencil-shaped, monotonous. There is intervening stroma between glands. The glandular contour is smooth E) 40x histology showing shows papillary fronds of the lesion
Figure: Figure 1: A/B: Esophagram showing fixed irregular segmental narrowing of the mid and distal esophagus, along with delayed esophageal transit. C: Low-dose CT showing a moderate-sized hiatal hernia and a diffusely fluid-distended esophagus. D: EUS of a fully circumferential, 3.52 cm thick isoechoic mucosal lesion
Disclosures: Sheel Patel indicated no relevant financial relationships. Endashaw Omer indicated no relevant financial relationships.
Sheel Patel, DO, Endashaw Omer, MD. P3019 - Atypical Presentation of Barrett's Esophagus: A 25 Cm Circumferential Polypoid Mass With Foveolar-Type Dysplasia, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.