Department of Medicine, George Washington University School of Medicine and Health Sciences Washington, DC
Zeina Bani Hani, MBBS1, Romy Chamoun, MD2, Simran Gupta, MD3, Robert S.. Gordon, DO, MS4, Jennie Zhang, DO5, Huimin Yu, MD, PhD6, Marie L. Borum, MD, EdD, MPH, FACG3 1Department of Medicine, George Washington University School of Medicine and Health Sciences, Washington, DC; 2George Washington University School of Medicine and Health Sciences, Washington, DC; 3Division of Gastroenterology and Liver Disease, Department of Medicine, George Washington University School of Medicine and Health Sciences, Washington, DC; 4George Washington University School of Medicine and Health Sciences, Arlington, WA; 5George Washington University, Washington, DC; 6George Washington University Hospital, Washington, DC Introduction: Zolbetuximab is a novel chimeric monoclonal antibodythat is used in patients with advanced gastric or gastro-esophageal junction (G/GEJ) adenocarcinoma.It targets Claudin 18.2 is a protein that is often overexpressed in gastric and GEJ cancers.Acute diarrhea is a recognized adverse reaction associated withZolbetuximab.We presentthe first documentedcase of a female with poorly differentiated gastric adenocarcinoma that developed acutecolitiscomplicated by perforationafterinitiation of Zolbetuximab.
Case Description/
Methods: An85-year-old female withhistory of hypertension, atrial fibrillation, mitral regurgitation, congenital hypertriglyceridemia,osteoporosis, and moderately to poorly differentiated adenocarcinoma of the stomach diagnosed4 months prior to admission. Shewason standard chemotherapy “FOLFOX”and developed acuteprofusewatery diarrheaafter addition of Zolbetuximab.Shereported12-15 bowel movements daily after starting Zolbetuximab.Stool studies for gastrointestinal infections were negative. Abdominal CTwasnotablefor contained rectal wall perforation, pneumatosis intestinalis in the transverse colon,andhyperemicappearance of small-bowel loops, concerning for enteritis.The diarrhea persisted through scheduled Lomotil, Loperamide, and cholestyramine.Arepeat abdominal CT demonstratingspontaneousresolution oftherectal perforation and interval decrease ofthe transverse colonpneumatosis.Sigmoidoscopywith water immersionwasnotable foran ulcer located in the transverse colon andsevere localized inflammation of the sigmoid colonand diverticulosiswithbiopsy demonstratingacute inflammation,negative for CMV.Hersymptomsgraduallyimproved with conservative management. Discussion: The most common adverse reactionsinpatientsonzolbetuximab with chemotherapyarenausea, vomiting, fatigue, and diarrhea.Management of Zolbetuximab-inducedacute diarrhea involves supportive care, including assessment of severity, correction of fluid and electrolyte imbalances, and antidiarrheal agents as clinically indicated.Given the onset of symptoms shortly after initiation of zolbetuximabwithout evidence of infection, this caserepresentszolbetuximab-induced colitis complicated withcolonic perforation which is not a well-documented adverse reaction.This is a potentially serious complicationto a novel agentwhich may require further evaluation in phase IV clinical trialsand monitoring in clinical practice.
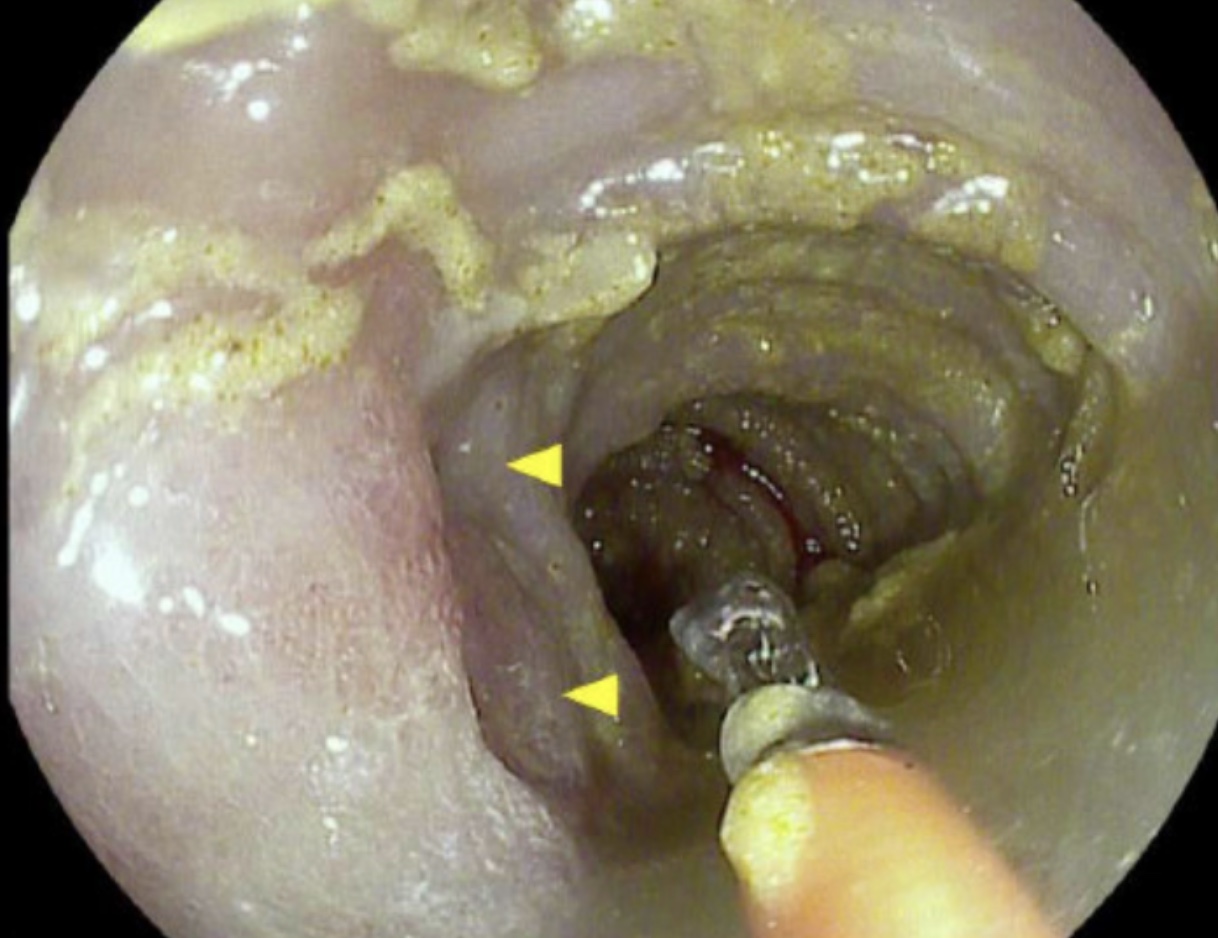
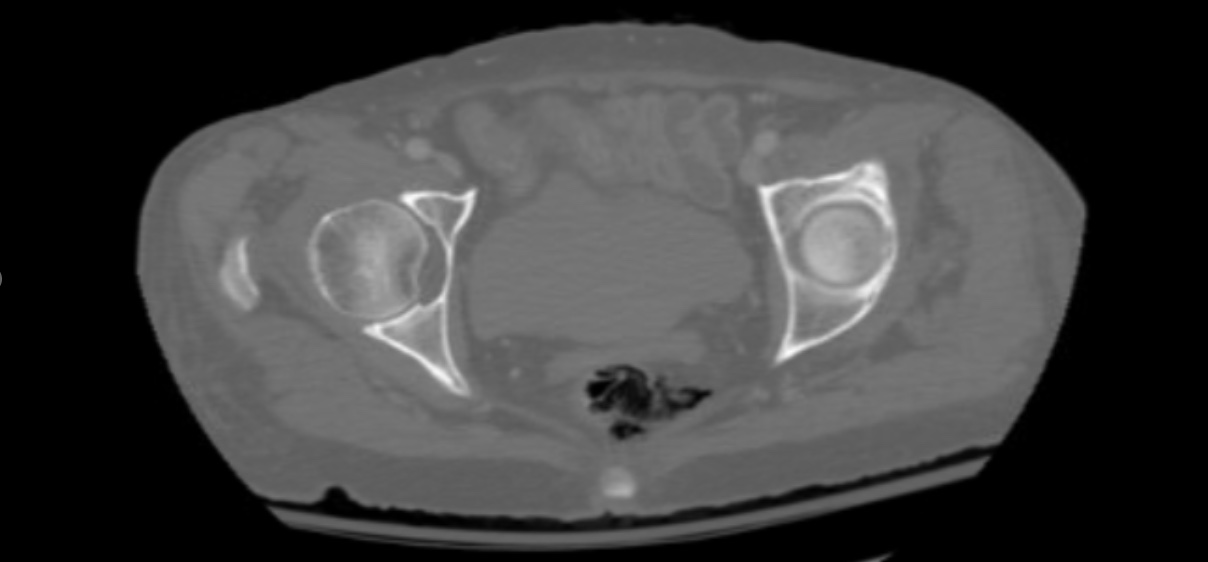
Figure: There is discontinuity of the left lateral rectal wall with surrounding free air