Aakriti Soni, MD1, Bilal Ashraf, MD2, Galvin Dhaliwal, MD3, Ahmed Ouni, MD3 1HCA Houston Healthcare Kingwood, Kingwood, TX; 2HCA Healthcare Kingwood Hospital/University of Houston, Kingwood, TX; 3HCA Healthcare, Kingwood, TX Introduction: Dedifferentiated liposarcoma (DDL) is a rare and aggressive subtype of liposarcoma. Even more rare is a significant involvement of the gastrointestinal tract by dedifferentiated liposarcoma. Due to its rarity, DDL poses diagnostic and therapeutic challenges.
Case Description/
Methods: A 52-year-old male with an unremarkable history presented to the emergency department with a 4-day history of abdominal pain, nausea, and intermittent vomiting. He reported an unintentional weight loss of approximately 8 pounds over the past three months. Family history was notable for colon cancer in his father, however he had never undergone colorectal cancer screening. CT scan of the abdomen and pelvis revealed a 3.5 cm mass within the proximal transverse colon, raising concern for a primary colonic neoplasm. A 4.4 cm adjacent soft tissue mass was identified, initially interpreted as metastatic lymphadenopathy. Subsequent upper endoscopy was unremarkable. Colonoscopy revealed a frond-like, villous, non-obstructive lesion measuring approximately 5 cm in the proximal transverse colon. An attempt at endoscopic mucosal resection (EMR) was made but was unsuccessful. In a multidisciplinary decision involving colorectal surgery and gastroenterology teams, the patient was taken for a robotic-assisted laparoscopic extended right hemicolectomy with en bloc resection of the pericolonic mass and 20 regional lymph nodes. Histopathological evaluation demonstrated that the colonic lesion was a tubulovillous adenoma with no evidence of high-grade dysplasia or invasive carcinoma. Surprisingly, the adjacent mass was not nodal in origin but rather a DDL arising from a well-differentiated liposarcoma (WDL). Immunohistochemical staining was strongly positive for MDM2 amplification, confirming the diagnosis. All twenty lymph nodes were negative for malignancy. Given the complete surgical resection and the absence of nodal or distant spread, the multidisciplinary tumor board recommended surveillance without adjuvant chemotherapy or radiotherapy. Discussion: When radiographic examination shows a perigastrointestinal or retroperitoneal fatty mass and/or stranding of the fat adjacent to a solid gastrointestinal mass, this unusual scenario should be considered in the radiologic differential diagnosis. Treatment usually depends on resectability. In cases where size is too large for surgical intervention, neo-adjuvant chemotherapy is recommended for size reduction along with neo-adjuvant radiation to decrease local recurrences.
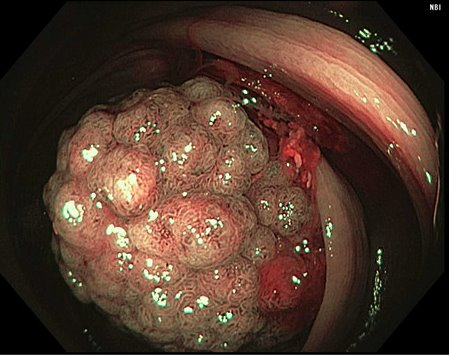
Figure: A frond-like, villous non-obstructing lesion found in the transverse colon on colonoscopy
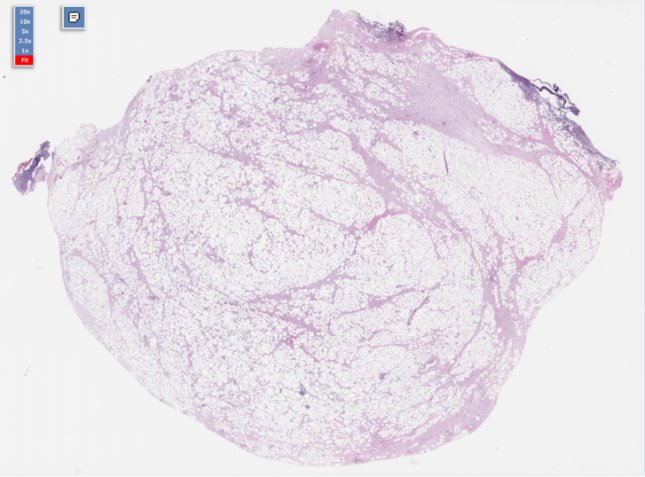
Figure: HPE showing a de-differentiated liposarcoma arising from a well-differentiated liposarcoma
Disclosures: Aakriti Soni indicated no relevant financial relationships. Bilal Ashraf indicated no relevant financial relationships. Galvin Dhaliwal indicated no relevant financial relationships. Ahmed Ouni indicated no relevant financial relationships.
Aakriti Soni, MD1, Bilal Ashraf, MD2, Galvin Dhaliwal, MD3, Ahmed Ouni, MD3. P2525 - A Curious Case of the Colon Cancer Mimic, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")