Harleen Chela, MBBS, MD1, Nisar Amin, MD2, Ebubekir Daglilar, MD2 1West Virginia University Charleston Area Medical Center, South Charleston, WV; 2Charleston Area Medical Center, Charleston, WV Introduction: Colorectal cancer remains as one of the most common cancers that are diagnosed and remains as significant contributor to morbidity and mortality. Despite advances in techniques, improving access to diagnostic modalities and increasing awareness, it often presents at a later stage and can recur despite treatment. Recurrence can be variable and can occur years after treatment. Liver is the most common location for metastasis to occur. We present an unusual case of recurrent colorectal cancer that occurred several years post treatment and presented as an isolated metastasis to the hilum of the liver leading to biliary obstruction without any other identifiable lesions including in the colon itself.
Case Description/
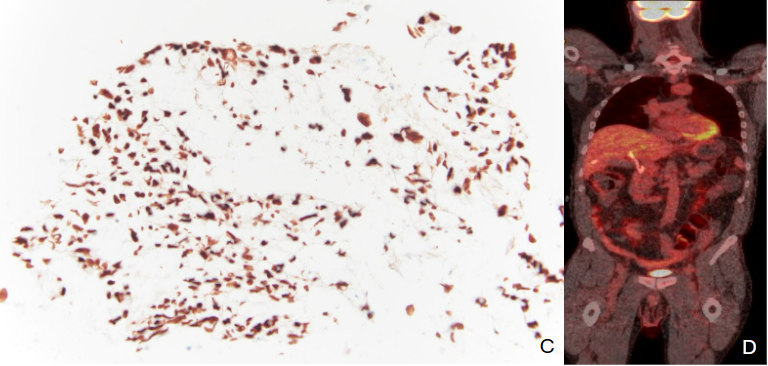
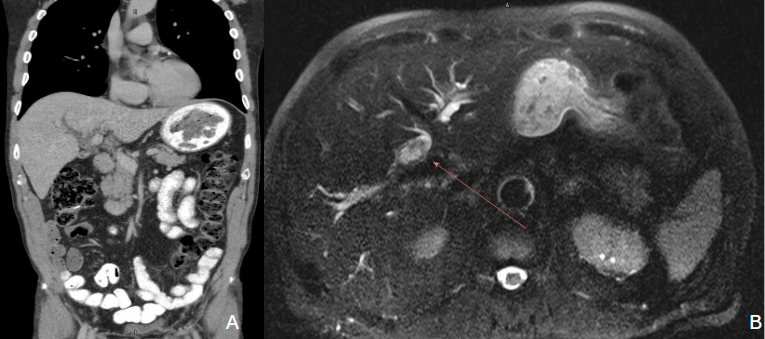
Methods: 68-year-old male with prior mucinous adenocarcinoma of the rectosigmoid (pT3N1b, 2017) treated with rectosigmoidectomy and adjuvant chemotherapy, and another primary mucinous adenocarcinoma of the cecum/appendix (2021) treated with segmental colectomy, appendectomy, and chemotherapy, presented to the ED with jaundice and elevated liver enzymes. A recent high-quality colonoscopy 3 months prior showed only three diminutive tubular adenomas.On exam, he appeared frail and cachectic with scleral icterus and bradycardia. RUQ tenderness was present. Labs revealed bilirubin 3.4 mg/dL, ALP 230 U/L, ALT 215 U/L, AST 95 U/L. Prior liver function tests from a few months prior were normal. CT abdomenrevealed severe intrahepatic biliary dilation with a suspected lesion at the common hepatic duct; the distal common bile duct was normal in caliber (Figure A). MRI/MRCP identified a soft tissue mass at the biliary confluence with no focal hepatic lesions (Figure B). Small 4 mm stable subpleural lung nodule seen previously was unchanged.Due to concerns about ERCP complications, patient opted for external biliary drainage by interventional radiology, during which cytology samples were obtained. Pathology revealed adenocarcinoma with immunohistochemistry positive for CK20 and CDX2 and negative for CK7, consistent with colorectal origin (Figure C). PET-CT revealed no definitive FDG uptake suggestive of malignancy or other active disease (Figure D). Medical and surgical oncology teams were consulted and he is pursuing further care at dedicated pancreaticobiliary center. Discussion: Metastatic adenocarcinoma of colon presenting as an isolated hilar mass is extremely rare and can mimic cholangiocarcinoma. Accurate diagnosis requires high clinical suspicion and tissue confirmation to guide management.
Figure: Figure A: CT abdomen revealed severe intrahepatic bile duct dilatation with suspected abnormality at the level of the common hepatic duct. The distal common bile duct was normal in caliber. Figure B: MRI/MRCP showed intrahepatic biliary duct dilatation with a soft tissue lesion seen at the hilum branch point between the right and left biliary system.
Figure: Figure C: Immunohistochemical stain showing tumor cells to be positive for CK20 and CDX2, and negative for CK7 favoring a colorectal source of origin. Figure D: A PET-CT scan showing no definitive evidence of malignancy.
Disclosures: Harleen Chela indicated no relevant financial relationships. Nisar Amin indicated no relevant financial relationships. Ebubekir Daglilar indicated no relevant financial relationships.
Harleen Chela, MBBS, MD1, Nisar Amin, MD2, Ebubekir Daglilar, MD2. P2514 - Hilar Mass Presenting as Isolated Colorectal Cancer Metastasis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.