Christina Joya, DO1, Christopher Pace, DO1, Cameron Yen, DO1, Zaheer Siddiqui, DO1, Melanie De Shadarevian, DO1, Scott Silver, DO1, Shahid Wahid, MD2, Vishvinder Sharma, MD1 1Valley Hospital Medical Center, Las Vegas, NV; 2UNLV School of Medicine, Las Vegas, NV Introduction: Portal cholangiopathy (PC) occurs as a result of extrinsic obstruction of the biliary tract due to engorged collateral veins in the hepatic hilum. These collateral veins, called portal cavernoma, can form due to increased pressure in the setting of portal vein thrombosis (PVT). In 2-4% of patients with PC, end stage liver disease may result. We present a case of a patient with PC and subsequent sequelae of end stage liver disease.
Case Description/
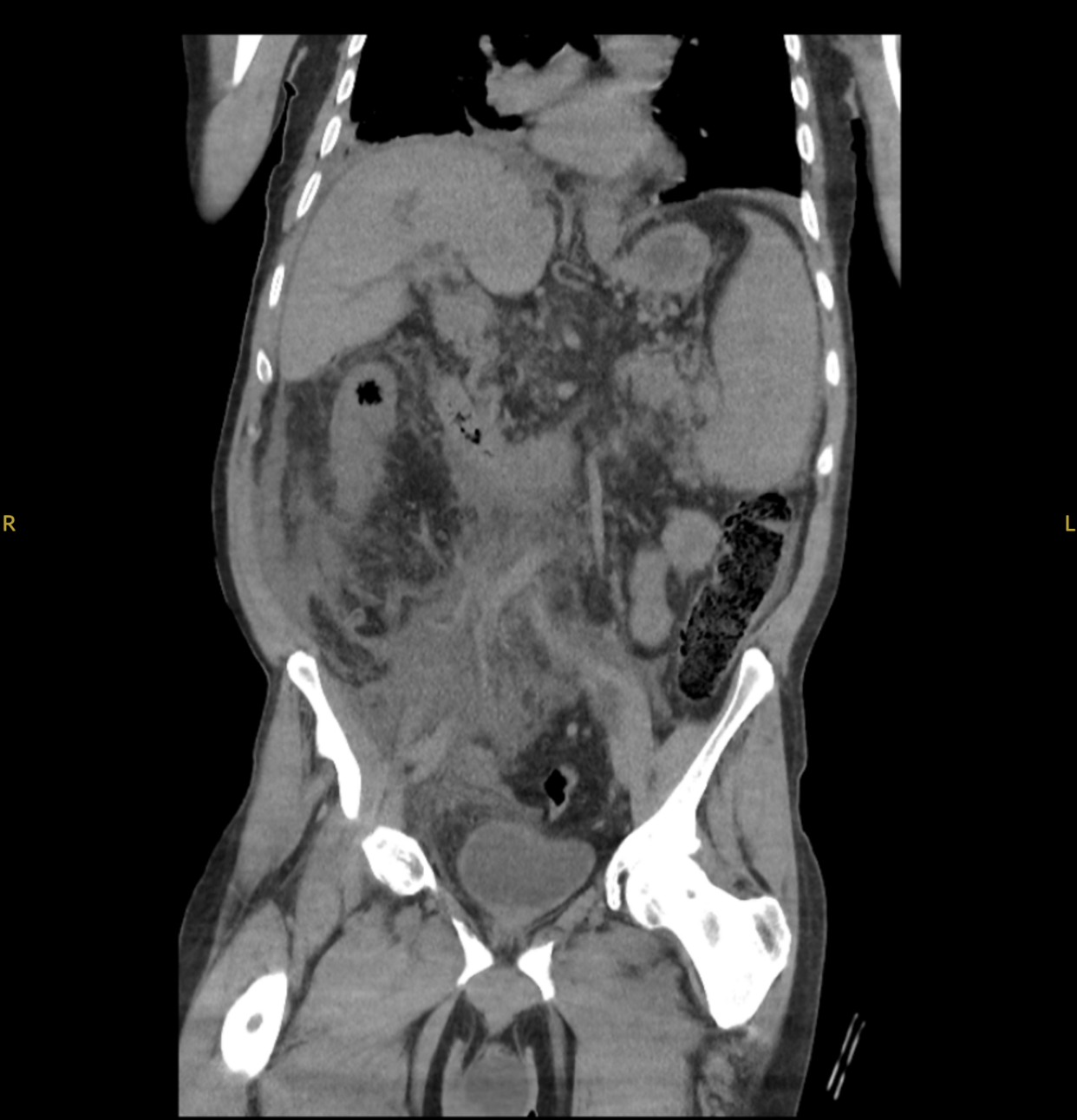
Methods: A 68 year old male presented for evaluation of elevated total bilirubin. MRI abdomen revealed a 4.4 x 3.9 cm x 5.6 cm periportal mass encasing the extrahepatic common bile duct with biliary obstruction, cirrhotic liver, splenomegaly, and splenic varices with a splenorenal shunt. EGD/ERCP/EUS revealed Grade 4 esophageal varices status post EVL, portal hypertensive gastropathy, and a 2.5 cm porta hepatis lesion compressing the CBD. Doppler studies revealed the lesion was vascular and no FNA was performed. Sphincterotomy and spyglass cholangioscopy showed varices within the bile duct without a mass, consistent with PC. Post procedure, the patient developed abdominal pain, nausea, vomiting, and lipase of 3040. CT abdomen/pelvis without contrast showed chronic PVT, cavernous transformation, biliary ductal dilation, and narrowing at the hepatic duct confluence from extrinsic compression by the cavernous transformation of the main portal vein versus involvement from the soft tissue mass extending from the pancreatic head to the porta hepatis. The patient was noted to be hepatitis B core Ab and surface Ab positive. A repeat EUS was done with biopsy of the mass consistent with benign pancreatic tissue with a component of collateral vessels. It was suspected that the etiology of the patient’s portal hypertension was primarily due to PVT and cavernous formation. The patient was found to have a JAK2 mutation. Discussion: While uncommon, PC must be considered in patients presenting with sequelae of end stage liver disease without clear etiology and or patients presenting with biliary masses. Early intervention of PC with portosystemic shunt decompression, or in severe cases hepaticojejunostomy or liver transplant, may decrease mortality and complication rates. The underlying cause of PC requires careful investigation. In cases of PVT and cavernous transformation, hypercoagulability workup is advised. Cases of JAK2 point mutation and myeloproliferative dysfunction leading to PC and associated advanced cirrhosis have been noted.
Figure: CT of the abdomen/pelvis showing cavernous transformation of the portal vein.
Disclosures: Christina Joya indicated no relevant financial relationships. Christopher Pace indicated no relevant financial relationships. Cameron Yen indicated no relevant financial relationships. Zaheer Siddiqui indicated no relevant financial relationships. Melanie De Shadarevian indicated no relevant financial relationships. Scott Silver indicated no relevant financial relationships. Shahid Wahid indicated no relevant financial relationships. Vishvinder Sharma indicated no relevant financial relationships.
Christina Joya, DO1, Christopher Pace, DO1, Cameron Yen, DO1, Zaheer Siddiqui, DO1, Melanie De Shadarevian, DO1, Scott Silver, DO1, Shahid Wahid, MD2, Vishvinder Sharma, MD1. P2321 - Cavernous Transformation of the Portal Vein Mimicking a Biliary Mass in a JAK2-Positive Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.