Muhammad S. Abbas, MBBS, MD1, Scott Diamond, DO2 1Valley Health System, Las Vegas, Las Vegas, NV; 2Utah Gastroenterology, St. George, UT Introduction: Iatrogenic pancreatic duct injury is a rare but serious complication of left nephrectomy, particularly in the setting of dense retroperitoneal adhesions. Disruption of the pancreatic duct may lead to significant morbidity including external pancreatic fistula, pseudocyst formation and portosplenic venous thrombosis.
Case Description/
Methods: 53-year-old male with ankylosing spondylitis and recurrent left ureteropelvic junction obstruction complicated by recurrent pyelonephritis, underwent open left nephrectomy. Intraoperatively, dense adhesions and scar tissue involving the spleen and pancreatic tail were encountered due to patient's history of recurrent infections. Three months postoperatively, the patient developed a large retroperitoneal fluid collection (13×13×16 cm), which was initially managed with percutaneous drainage. However, following eventual removal of the drains approximately five months post-op, recurrent collections ensued requiring JP drain to be replaced. Further workup including fluid analysis revealed markedly elevated amylase ( >7500 U/L) and lipase ( >3000 U/L), consistent with pancreatic leak. MRCP done at the time demonstrated a thick-walled collection near the pancreatic tail without overt ductal dilation or parenchymal injury, and resolution of fluid collection was noted after drain replacement on subsequent imaging. At 9 months post-op, patient had a followup CT abdomen pelvis with contrast which revealed an isolated remnant of the distal pancreatic tail with a disconnected pancreatic duct, consistent with Disconnected Pancreatic Duct Syndrome (DPDS), along with a persistent pseudocyst (4.8×2.7×5 cm) and chronic splenic vein thrombosis. Development of collateral circulation around the splenic hilum and gastric wall was noted, indicating evolving sinistral (left-sided) portal hypertension with isolated gastric varices. Discussion: This case highlights a rare but significant complication of left nephrectomy: iatrogenic pancreatic duct injury leading to Disconnected Pancreatic Duct Syndrome. Early recognition and multidisciplinary management involving gastroenterology, interventional radiology, and surgery are essential to prevent long-term morbidity. Pancreatic duct injury should be considered in patients with persistent high-amylase fluid collections following left-sided retroperitoneal surgery. Disconnected Pancreatic Duct Syndrome is a challenging postoperative complication with potential for serious vascular and gastrointestinal sequelae.
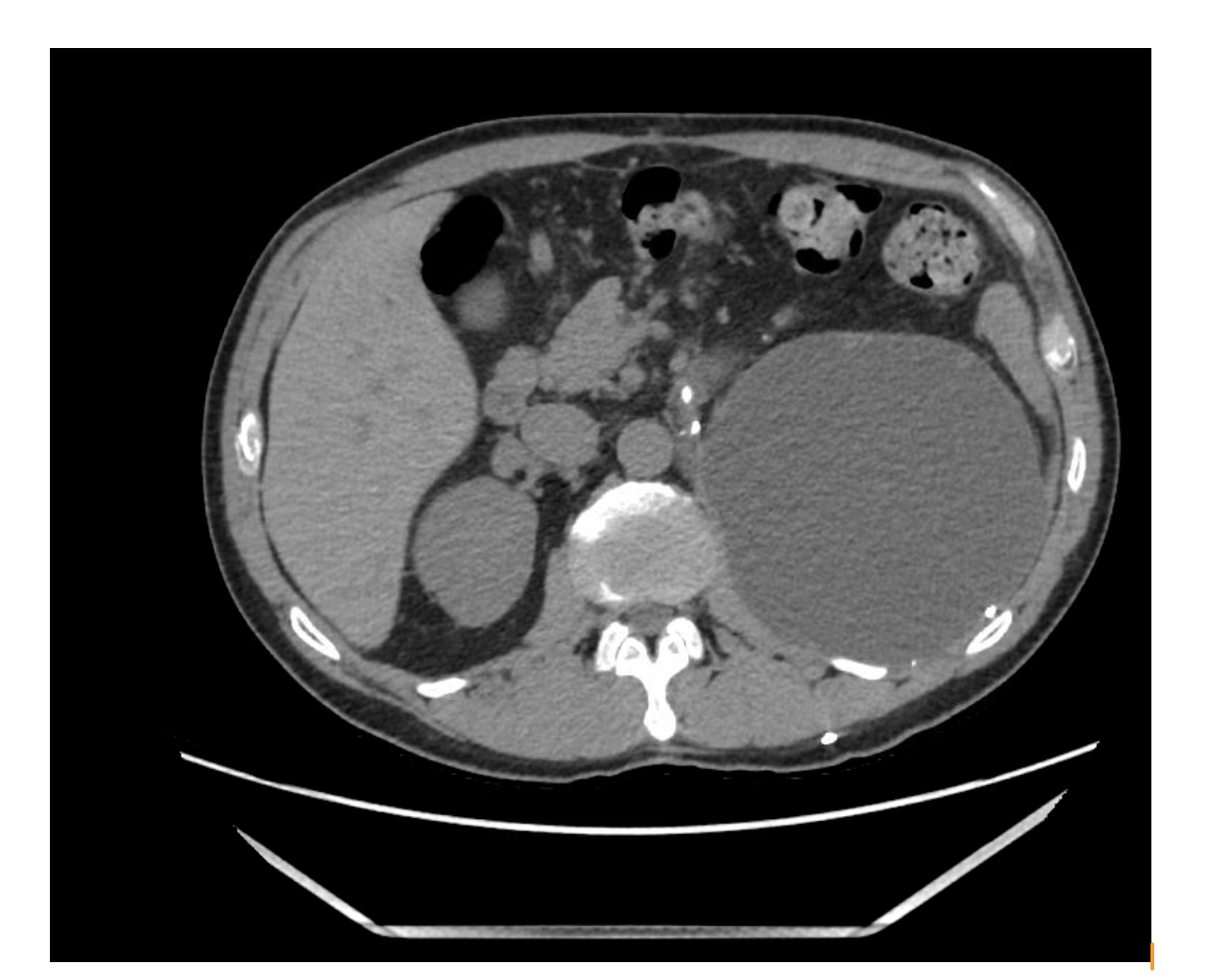
Figure: CT abdomen pelvis with contrast showing retroperitoneal fluid collection 3 month post operatively
Figure: CT abdomen pelvis with contrast showing pancreatic pseudocyst, 9 months post operatively
Disclosures: Muhammad Abbas indicated no relevant financial relationships. Scott Diamond indicated no relevant financial relationships.
Muhammad S. Abbas, MBBS, MD1, Scott Diamond, DO2. P2260 - Iatrogenic Pancreatic Duct Injury Following Left Nephrectomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.