University of Iowa Hospitals & Clinics Iowa City, IA
Sayed Tauseef Ahmad Jan, MD1, Munish Ashat, MD1, Shifa Kakakhel, MD2, Shahryar khan, MD3 1University of Iowa Hospitals & Clinics, Iowa City, IA; 2Khyber Medical University, Peshawar, North-West Frontier, Pakistan; 3University of Kansas Medical Center, Kansas City, KS Introduction: Pancreatic mixed neuroendocrine–non-neuroendocrine neoplasms (MiNENs) are rare, aggressive malignancies characterized by the presence of both a neuroendocrine component, typically a poorly differentiated neuroendocrine carcinoma (PDNEC), and a non-neuroendocrine component, usually adenocarcinoma, each comprising ≥30% of the tumor. They are associated with poor prognosis. Their rarity, histologic heterogeneity, and limited clinical data can present diagnostic and therapeutic challenges.
Case Description/
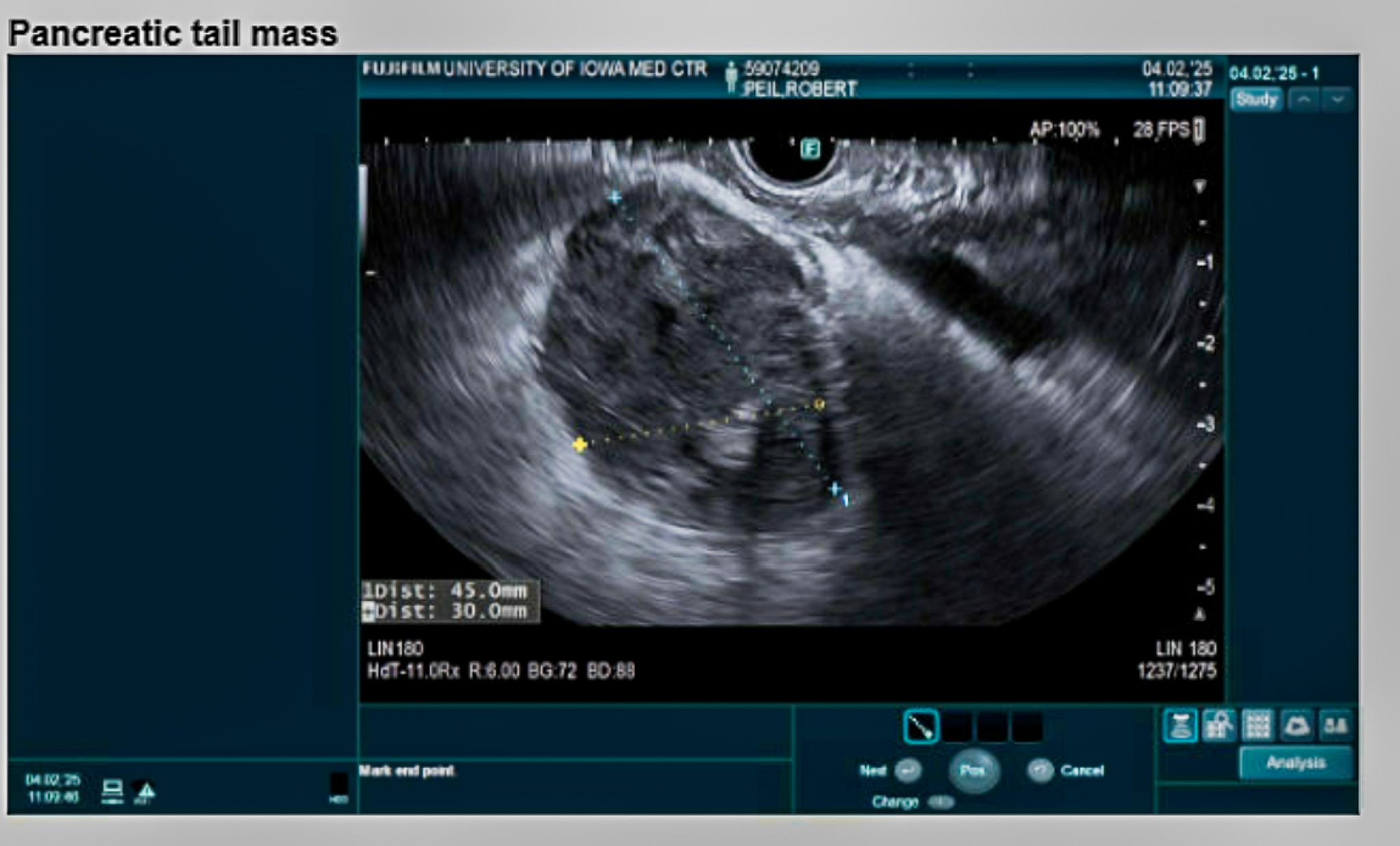
Methods: A 75-year-old male with a history of coronary artery disease, stroke, and dementia presented with severe abdominal pain and decreased appetite for two weeks. CT of the abdomen and pelvis revealed a 4 cm mass in the pancreatic tail. A 2.2 cm nodule in the right lung and two small hepatic lesions were also noted. Endoscopic ultrasound demonstrated a hypoechoic mass with irregular borders. Pathology showed poorly differentiated carcinoma with mixed acinar and neuroendocrine features. Surgical oncology evaluated the patient and deemed him a high risk surgical candidate. The family opted against surgical resection. He was discharged with follow-up with medical oncology. He underwent CT-guided biopsy of the right lower lobe (RLL) lesion, which was non-diagnostic due to insufficient tissue sample. He is currently planned for PET-CT imaging for staging. Discussion: Pancreatic MiNENs account for approximately 0.5% of pancreatic adenocarcinomas and 5% of pancreatic neuroendocrine neoplasms. Acinar-type carcinomas with neuroendocrine components are exceedingly rare. Diagnosis requires immunohistochemical confirmation of both neuroendocrine (chromogranin, synaptophysin) and acinar (BCL-10) markers. Due to limited clinical data, management remains ill-defined. Surgical resection is the mainstay for non-metastatic disease. If adjuvant therapy is indicated or the tumor is unresectable, treatment typically targets the more aggressive component. In most cases, regimens follow protocols for gastroenteropancreatic neuroendocrine carcinomas (GEP NECs). When the neuroendocrine component is NEC, platinum-based chemotherapy is often used. Alternatively, gastrointestinal adenocarcinoma regimens such as FOLFOX or FOLFIRINOX may be considered, though supporting data remain limited. This case report underscores the need for further research to establish standardized treatment protocols for this rare and aggressive group of tumors.
Figure: Endoscopic Ultrasound Image of the Pancreatic tail mass
Disclosures: Sayed Tauseef Ahmad Jan indicated no relevant financial relationships. Munish Ashat indicated no relevant financial relationships. Shifa Kakakhel indicated no relevant financial relationships. Shahryar khan indicated no relevant financial relationships.
Sayed Tauseef Ahmad Jan, MD1, Munish Ashat, MD1, Shifa Kakakhel, MD2, Shahryar khan, MD3. P4521 - Mixed Neuroendocrine-Non-Neuroendocrine Neoplasm (MiNEN) of the Pancreas: A Rare Diagnostic and Therapeutic Challenge, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.