Rida Aziz, DO1, Evan Daugherty, MD2, Andre Gabriel, MD3 1Inspira Health Network, Glassboro, NJ; 2Inspira Health Network, Mullica Hill, NJ; 3Inspira Medical Center Mullica Hill, Mullica Hill, NJ Introduction: Pancreatic pseudoaneurysms can follow incidental surgical manipulation of the pancreas and can result in complications including gastric outlet obstruction (GOO). Pseudoaneurysms causing GOO are typically managed via endovascular embolization, with a low risk of recurrence and occasionally require surgical intervention. Post-operative pseudoaneurysms are often described but generally occur within weeks of manipulation. We describe a case of pancreatic pseudoaneurysm occurring 6 years following cholecystectomy, causing GOO and requiring embolization and subsequent surgery following persistent GOO.
Case Description/
Methods: A 60-year-old female initially presented to the hospital with nausea and vomiting. Imaging of the abdomen demonstrated a 3.1x2.3 cm pseudoaneurysm with irregularity to the distal duodenum. She had no history of pancreatitis, trauma, alcohol use or sequela of pancreatitis. Her only notable history was a open cholecystectomy approximately 6 years prior. She underwent successful coiling of the pseudoaneurysm via the inferior pancreaticoduodenal artery. She was discharged home, only to return two weeks later with similar symptoms. Repeat imaging demonstrated persistent pseudoaneurysm with residual hemorrhage resulting in mass effect on the 2nd and 3rd portions of the duodenum. An EGD was performed, however the endoscope was unable to transverse the obstruction and the patient ultimately underwent retrocolic isoperistaltic gastrojejunostomy. She was able to be discharged home shortly after with no complications. Biopsies obtained on EGD showed inflamed but otherwise normal mucosa. Discussion: Surgical manipulation of the pancreas is well known to cause pancreatic complications. Although not common after cholecystectomy, our pseudoaneurysm is presumed to have formed following manipulation at that time. Alternative etiologies including simple idiopathic pseudocysts are entertained. Post-operative pseudocyst is most described following pancreatic surgeries, commonly presenting after a period of weeks. Symptoms most often include abdominal pain or anorexia, but in cases of resultant GOO can include nausea and vomiting. Our case is presumed to have been indolent for a period of years before finally causing symptoms after the patient developed GOO. Recurrence after embolization is a common occurrence. Our case illustrates the importance of clinicians considering pseudoaneurysm in the differential for patients with appropriate symptoms and any prior surgery in proximity to the pancreas.
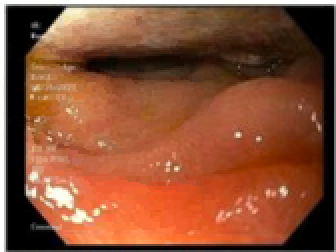
Figure: Significant luminal narrowing in second part of the duodenum, concern for extrinsic compression.
Disclosures: Rida Aziz indicated no relevant financial relationships. Evan Daugherty indicated no relevant financial relationships. Andre Gabriel indicated no relevant financial relationships.
Rida Aziz, DO1, Evan Daugherty, MD2, Andre Gabriel, MD3. P4515 - Challenging Case of Pancreatic Pseudoaneurysm Due to Distant Cholecystectomy Causing Persistent Gastric Outlet Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.