University of Pittsburgh Medical Center Harrisburg, PA
Angsupat Pornchai, MD1, Hajra Khan, MD1, Adil Mir, MD2, Nicha Wongjarupong, MD3 1University of Pittsburgh Medical Center, Harrisburg, PA; 2Augusta Health, Fishersville, VA; 3Cedars-Sinai Medical Center, Los Angeles, CA Introduction: Delay in cholecystectomy for gallbladder masses significantly increases the risk of carcinoma; timely removal is essential to prevent malignant transformation and improve patient prognosis.
Case Description/
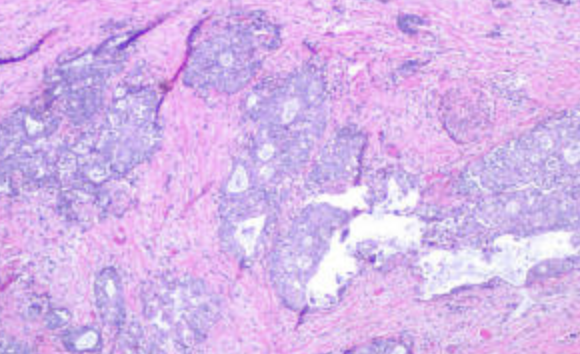
Methods: A 78-year-old woman with a history of chronic obstructive pulmonary disease on 4 L/min of baseline oxygen, hypothyroidism, extensive cholelithiasis, and a suspected gallbladder neoplasm on imaging—who had received a Wallflex metal stent 7 months earlier for a benign distal common bile duct stricture—was lost to follow-up after an outpatient cholecystectomy was recommended. She re-presented with sepsis and altered mental status: fever (104 °F), tachypnea, tachycardia, leukocytosis (26,000/µL), and cholestatic features (ALP 430 U/L; total bilirubin 4.3 mg/dL). Endoscopic retrograde cholangiopancreatography (ERCP) demonstrated duodenal compression by a distended gallbladder and occlusion of the stent by debris, without an identifiable mass. Contrast-enhanced computed tomography confirmed a hydropic gallbladder with gallstones. A magnetic resonance imaging (MRI) performed 7 months earlier had shown a 4 × 3 cm ill-defined lesion at the gallbladder fundus, with focal narrowing of the Phrygian cap and associated enhancement. She underwent laparoscopic cholecystectomy and repair of a newly identified cholecystoduodenal fistula. Pathology revealed a moderately differentiated adenocarcinoma (stage T3) in the fundus, with possible adenocarcinoma at the fistula site. She was not a candidate for adjuvant chemotherapy due to poor performance status and multiple comorbidities. Discussion: Gallbladder polyps ≥ 1 cm have reported malignancy rates of 6–8.5%; current guidelines recommend cholecystectomy for lesions ≥ 1 cm or in symptomatic patients. Fundal lesions on MRI warrant expedited surgical evaluation, particularly in high-risk individuals. This case illustrates how noncompliance with outpatient follow-up and delayed intervention allowed progression to stage T3 adenocarcinoma.
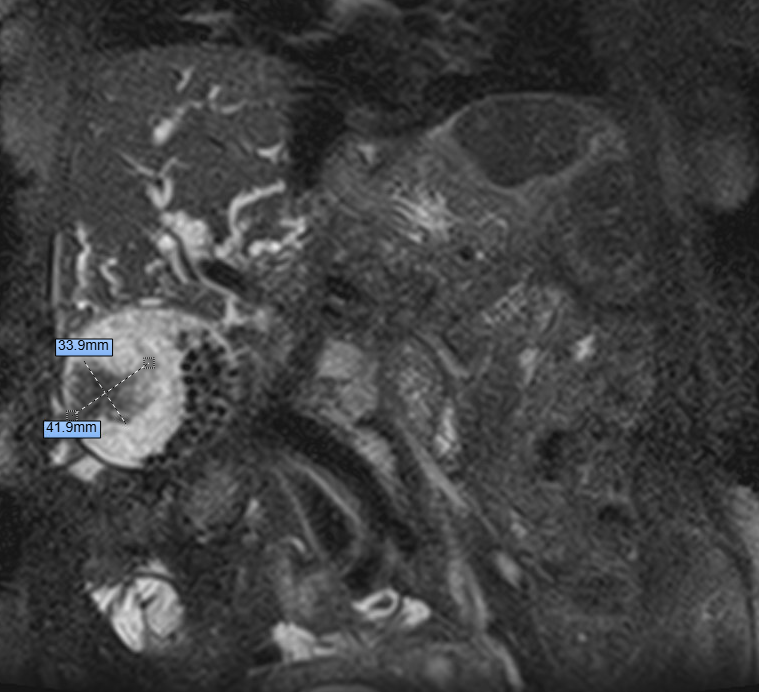
Figure: MRI abdomen with and without contrast shows multiple gallstones and an ill-defined, enhancing 4 × 3 cm mass-like lesion at the gallbladder fundus adjacent to a Phrygian cap, concerning for neoplasm with marked intra- and extrahepatic biliary dilation. The common bile duct measures 14 mm.
Disclosures: Angsupat Pornchai indicated no relevant financial relationships. Hajra Khan indicated no relevant financial relationships. Adil Mir indicated no relevant financial relationships. Nicha Wongjarupong indicated no relevant financial relationships.
Angsupat Pornchai, MD1, Hajra Khan, MD1, Adil Mir, MD2, Nicha Wongjarupong, MD3. P4514 - A 7-Month Delay in Cholecystectomy: Progression of a Gallbladder Mass to Stage T3 Cancer, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")