University of Miami Miller School of Medicine at JFK Medical Center Atlantis, FL
Panida Charnvitayapong, MD1, Juzer Ali Asgar, MD1, Bebika Subedi, MD1, Amit Sah, MD2 1University of Miami Miller School of Medicine at JFK Medical Center, Atlantis, FL; 2Larkin Community Hospital, Hialeah, FL Introduction: Von Hippel-Lindau (VHL) syndrome is a rare autosomal dominant disorder marked by the development of cysts and tumors across multiple organ systems. Pancreatic involvement occurs typically as asymptomatic cysts or neuroendocrine tumors, but complete replacement of the pancreas by cysts is exceedingly rare.
Case Description/
Methods: A 32-year-old woman with a history of VHL and major depressive disorder presented with worsening headaches and visual changes. She had previously been diagnosed with brain lesions under routine surveillance. Earlier in the year, interval growth led to a neurosurgical recommendation for resection, but she was unable to proceed due to insurance. On this admission, neuroimaging showed multiple enhancing brain lesions, including a dominant right parietal mass with significant vasogenic edema and smaller foci in the cerebellum. Concern for metastatic disease prompted abdominal imaging, which revealed multiple large pancreatic cysts. MRCP demonstrated near-total replacement of the pancreatic parenchyma. She reported mild epigastric pain but denied jaundice, chronic NSAID use, or stool changes. Labs showed mildly elevated liver enzymes with normal ALP and bilirubin. She was discharged with outpatient follow-up but returned soon after with worsening abdominal pain. ERCP with needle aspiration yielded thin, brown serous fluid consistent with pancreatic cysts. Cytology, tumor markers (CEA and CA 19-9), and PET imaging were negative for malignancy. The pancreatic disease was managed conservatively while neurosurgical evaluation continued for the CNS lesions. Discussion: VHL is caused by a germline mutation in the VHL tumor suppressor gene on chromosome 3. Loss of VHL protein function leads to the accumulation of hypoxia-inducible factors (HIFs), promoting angiogenesis and tumorigenesis. VHL-associated tumors may affect the CNS, retina, pancreas, kidneys, and adrenal glands. Pancreatic cysts are often incidental but occur in at least 75% of affected individuals. The pancreas is hypothesized to be especially susceptible to biallelic inactivation of the VHL gene in pancreatic progenitor or ductal cells. The diagnosis is clinical and supported by imaging and genetic testing. Management is typically conservative, with surveillance and intervention reserved for symptomatic or suspicious lesions.
This case presents an uncommon manifestation of VHL and emphasizes the importance of considering this syndrome and how to tailor care with a multidisciplinary approach.
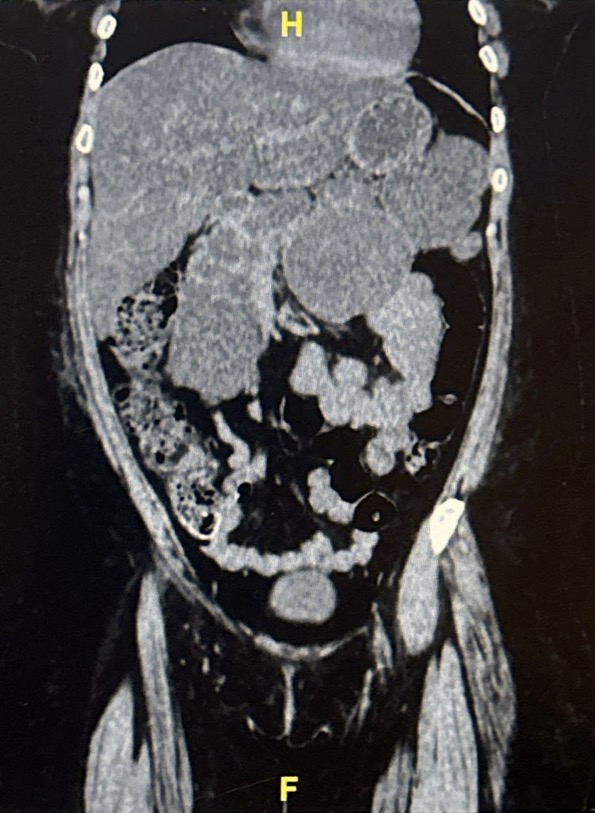
Figure: CT Abdomen/Pelvis (coronal): Multiple large cystic masses with diffuse architectural distortion to the pancreas
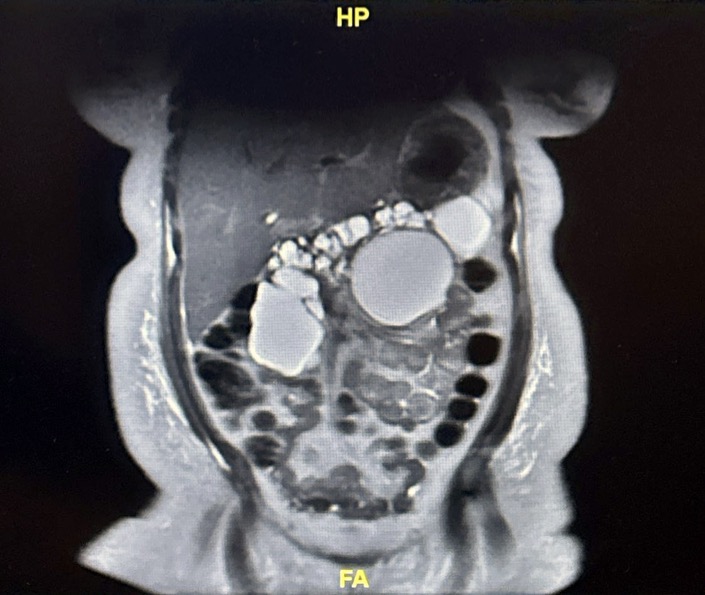
Figure: MRCP (coronal): Numerous cysts essentially replacing the pancreatic parenchyma
Disclosures: Panida Charnvitayapong indicated no relevant financial relationships. Juzer Ali Asgar indicated no relevant financial relationships. Bebika Subedi indicated no relevant financial relationships. Amit Sah indicated no relevant financial relationships.
Panida Charnvitayapong, MD1, Juzer Ali Asgar, MD1, Bebika Subedi, MD1, Amit Sah, MD2. P4507 - Extensive Von-Hippel-Lindau (VHL) Syndrome with Complete Pancreatic Involvement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")