Omar Shamaa, MD1, Jonathan A. Montrose, DO1, Maher Ghanem, MD2, Robert Pompa, MD1 1Henry Ford Health, Detroit, MI; 2Central Michigan University College of Medicine, Saginaw, MI Introduction: Cholangiocarcinoma is a rare malignancy of the biliary tree and the second most common primary liver tumor. It spreads via the lymphatic system to the liver, lung, bone, and brain. Here we report a rare case of cholangiocarcinoma with metastasis to the esophagus.
Case Description/
Methods: A 52-year-old male presented with unintentional weight loss, nausea and vomiting. Esophagogastroduodenoscopy (EGD) and endoscopic ultrasound (EUS) revealed a distal esophageal tumor extending 3 cm into the proximal stomach. Biopsies revealed adenocarcinoma and PET-CT was negative for metastases. He underwent an Ivor-Lewis esophagectomy four months later. The patient re-presented 32 months after surgical resection with right upper quadrant abdominal pain, vomiting and elevated liver enzymes (total bilirubin 17.7 mg/dL, direct bilirubin >10 mg/dL, alkaline phosphatase 627 U/L). Magnetic resonance cholangiopancreatography (MRCP) noted intrahepatic bile duct dilation without obstructive lesions. Repeat EGD showed an esophageal polyp at 35cm that was resected en bloc. Pathology was consistent with submucosal gland/duct adenoma. Endoscopic retrograde cholangiopancreatography (ERCP) failed to traverse the biliary stricture, therefore two percutaneous transhepatic external biliary drainage catheters (PTC) were placed into the right and left hepatic systems with LFT improvement. Follow up ERCP with direct cholangioscopy through the PTC sheath revealed a malignant stricture extending from the common hepatic to the right intrahepatic duct. This was treated with plastic stent placement and stricture biopsies confirmed invasive adenocarcinoma. The patient was subsequently found to have hepatic metastasis and was initiated on chemotherapy (gemcitabine, cisplatin and durvalumab). The initially acquired esophageal polyp resection sample was then re-evaluated and favored to be metastasis of a bile duct primary. Discussion: Metastasis of cholangiocarcinoma to the esophagus is exceedingly rare, with only two prior reports. This case had a unique presentation with an original unrelated primary esophageal cancer, followed by metastatic cholangiocarcinoma with esophageal involvement almost 3 years post-esophagectomy. This highlights the importance of considering metastatic disease in patients with atypical gastrointestinal symptoms and emphasizes the role of a multidisciplinary approach in managing complex cholangiocarcinoma cases.
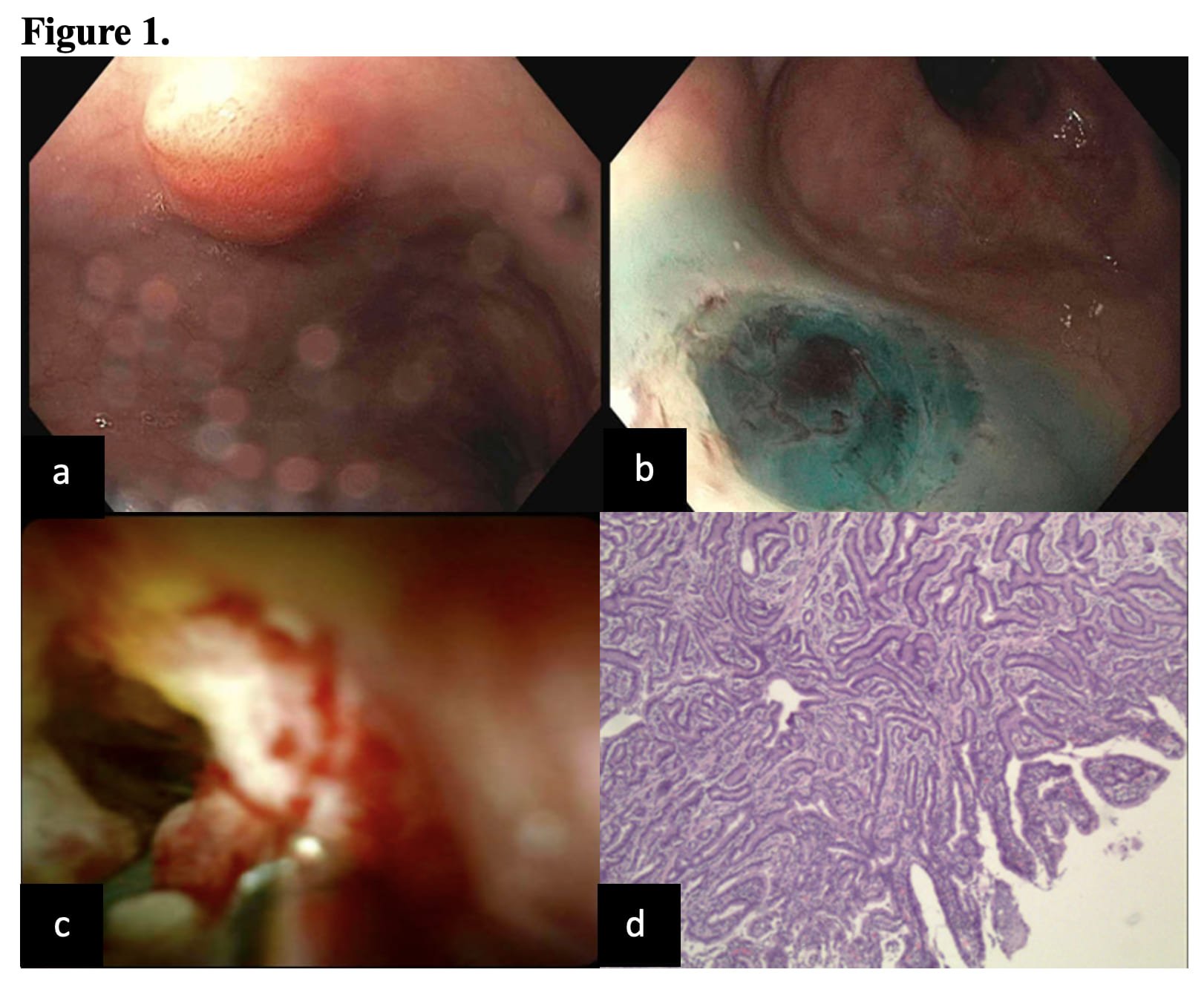
Figure: a. Distal esophageal polyp, b. Esophageal polyp site post-en bloc endoscopic mucosal resection (EMR), c. Cholangioscopy showing irregular biliary stricture with a mass-like projection and abnormal vessels. d. Esophageal polyp pathology showing exuberant adenomatous proliferation, favoring colonization of esophageal mucosa by a metastatic bile duct tumor.
Disclosures: Omar Shamaa indicated no relevant financial relationships. Jonathan Montrose indicated no relevant financial relationships. Maher Ghanem indicated no relevant financial relationships. Robert Pompa indicated no relevant financial relationships.
Omar Shamaa, MD1, Jonathan A. Montrose, DO1, Maher Ghanem, MD2, Robert Pompa, MD1. P4503 - Metastatic Cholangiocarcinoma Presenting as an Esophageal Polyp: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.