Corewell Health William Beaumont University Hospital Royal Oak, MI
Mujtaba Moazzam, MD1, Usman Bin Hameed, MD1, Aagamjit Singh, MBBS2, Ahmed Aref, MD1, Fady Banno, MD3 1Corewell Health William Beaumont University Hospital, Royal Oak, MI; 2William Beaumont Hospital, Troy, MI; 3Carewell Health William Beaumont Hospital, Royal Oak, MI Introduction: Endoscopic biliary stenting is a widely used intervention for biliary obstruction. Fully covered self-expandable metal stents (SEMS) offer prolonged patency but carry a higher risk of migration compared to plastic stents. Although often asymptomatic, stent migration can rarely cause serious complications. We report a case of small bowel obstruction (SBO) resulting from a distally migrated fully covered SEMS.
Case Description/
Methods: A 64-year-old male underwent laparoscopic cholecystectomy for gangrenous cholecystitis. He presented four weeks later with painless jaundice. Laboratory tests showed ALP 708 U/L, AST 64 U/L, ALT 728 U/L, total bilirubin 8.9 mg/dL, and direct bilirubin 6.4 mg/dL. Abdominal ultrasound revealed a dilated common bile duct (CBD) measuring 11 mm. Endoscopic ultrasound and ERCP confirmed choledocholithiasis. He underwent biliary sphincterotomy and stone removal, complicated by bleeding, followed by placement of a 10 mm × 6 cm fully covered SEMS. Within 24 hours, he developed abdominal distension and bilious vomiting. CT imaging revealed the stent had migrated into the proximal jejunum, causing a high-grade SBO. Emergent EGD did not visualize the stent, suggesting further distal migration. A second ERCP was performed for new stent placement and hemostasis. Conservative management with nasogastric decompression, IV fluids, and antibiotics was initiated. Serial KUB imaging over five days tracked the migrated stent as it progressed through the bowel to the rectum. His symptoms improved, and he was discharged in stable condition. Discussion: Biliary stent migration occurs in up to 10% of cases, with rates as high as 20% for fully covered metal stents. Risk factors include sphincterotomy, large-diameter CBDs, straight stent design, and recent surgery. Although most migrated stents pass spontaneously, fewer than 1% cause complications like SBO, usually when lodged in fixed or narrowed bowel segments, often due to adhesions. Our patient had multiple risk factors—a large, fully covered SEMS, recent sphincterotomy, and recent abdominal surgery—all predisposing to distal migration and obstruction. Conservative management with serial imaging often suffices, as in our case, where the stent eventually passed without intervention. Endoscopic or surgical intervention is reserved for complications or failure of expectant therapy. Prompt recognition and appropriate management are key to ensuring favorable outcomes while preserving the benefits of endoscopic stenting.
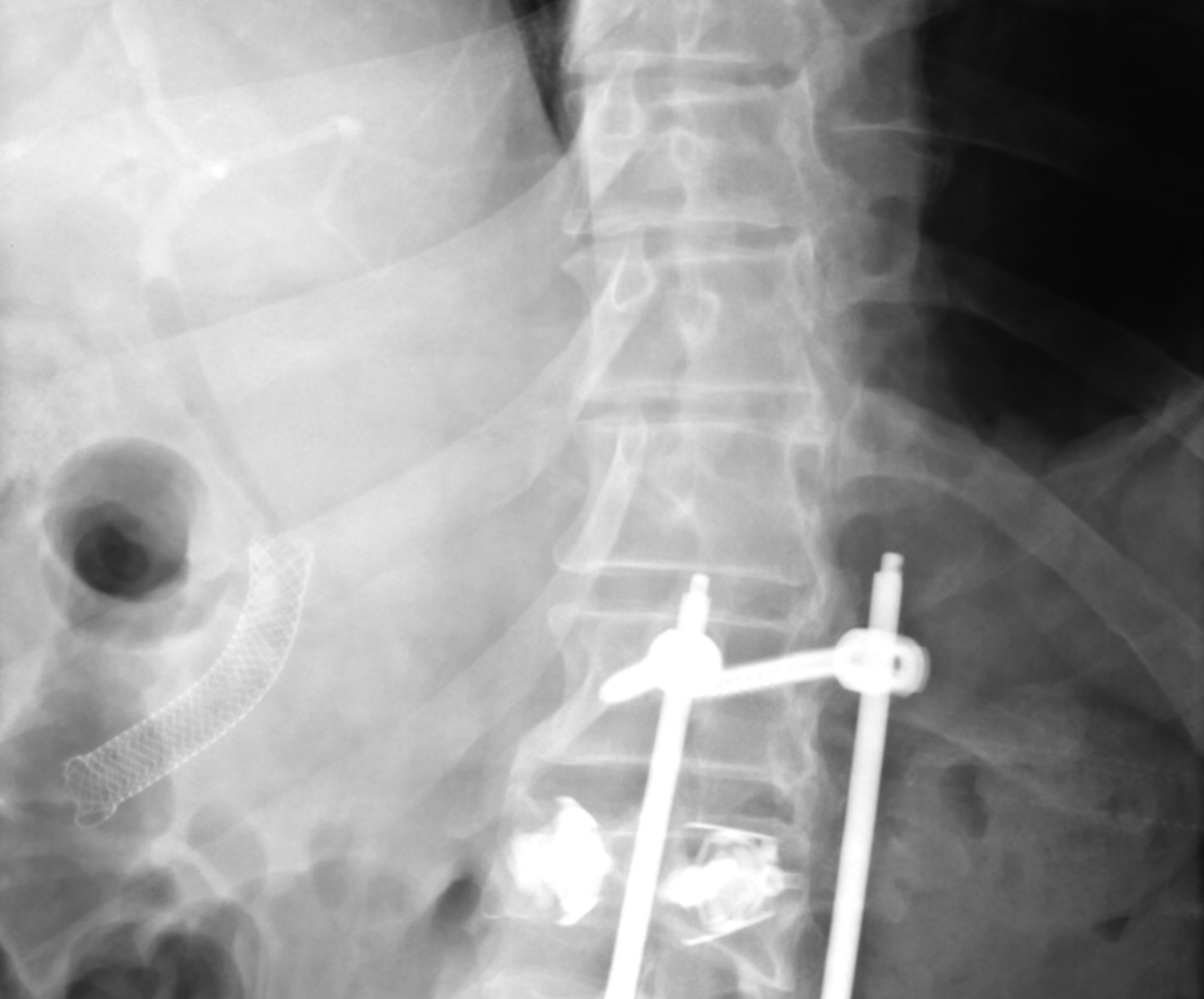
Figure: Fluoroscopic image demonstrating a 10 mm x 6 cm fully covered metal stent in the mid common bile duct
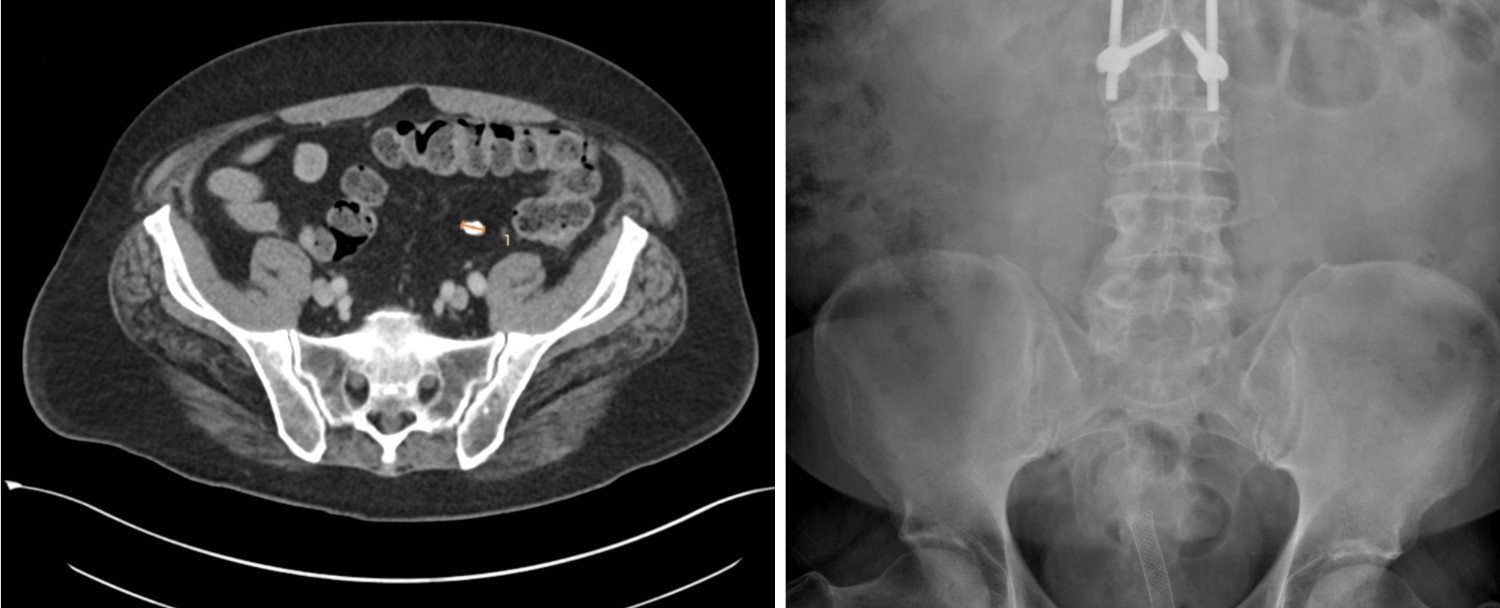
Figure: Left - CT abdomen demonstrating stent migration into the proximal jejunum; Right - Abdominal X-ray confirming stent migration into the rectum
Disclosures: Mujtaba Moazzam indicated no relevant financial relationships. Usman Bin Hameed indicated no relevant financial relationships. Aagamjit Singh indicated no relevant financial relationships. Ahmed Aref indicated no relevant financial relationships. Fady Banno indicated no relevant financial relationships.
Mujtaba Moazzam, MD1, Usman Bin Hameed, MD1, Aagamjit Singh, MBBS2, Ahmed Aref, MD1, Fady Banno, MD3. P4497 - Biliary Stent Migration Causing Small Bowel Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.