Ganesh Ramaprasad, MD, Angela Baquiran, MD, Chetan Pai, DO Mary Washington Healthcare, Fredericksburg, VA Introduction: Choledochoceles (type III choledochal cysts) account for approximately 2–5% of choledochal cysts and present with abdominal pain, pancreatitis, or cholangitis. Asymptomatic or “silent” cases are uncommon, and no documented association between choledochoceles and neurofibromatosis type 1 (NF1) exists. Early recognition is important to prevent complications such as pancreatitis or malignant transformation.
Case Description/
Methods: A 50-year-old female with asthma and NF1 presented following a syncopal episode. Labs revealed significantly elevated liver enzymes (AST 228 U/L, ALT 280 U/L, ALP 712 U/L) and mild lipase elevation (120 U/L) without pancreatitis symptoms. Previously, she had an isolated lipase elevation (1018 U/L) without clinical pancreatitis; outpatient evaluation was recommended but not completed due to lack of insurance. Chronic symptoms included severe nocturnal bile reflux characterized by frequent episodes of waking from sleep with heartburn and bilious emesis, which had been misdiagnosed and self-treated as severe GERD with over-the-counter medications. Magnetic resonance cholangiopancreatography (MRCP)demonstrated significant biliary dilation without evidence of obstructive lesions. Subsequent esophagogastroduodenoscopy confirmed a type III choledochocele.
Discussion: The majority of type III choledochal cysts (85–90 %) manifest with classical symptoms; presentation with isolated biochemical abnormalities without overt symptoms are rare, occurring in fewer than 10% of cases. Persistent bile reflux may be incorrectly attributed to GERD, delaying diagnosis. Although gastrointestinal involvement occurs in up to 25 % of individuals with NF1, biliary cystic lesions have not been previously reported in this population, making this the first documented case of an NF1-associated choledochocele. Clinicians should maintain a high index of suspicion for choledochoceles in patients with unexplained biochemical abnormalities and persistent upper gastrointestinal symptoms. Early identification allows for timely intervention, reducing the risk of pancreatitis and malignant transformation. This case highlights an atypical presentation of a type III choledochocele coexisting with NF1. To our knowledge, this is the first reported association. Recognition of subtle clinical and biochemical findings—especially in patients with underlying NF1—can facilitate earlier diagnosis and management, thereby improving outcomes.
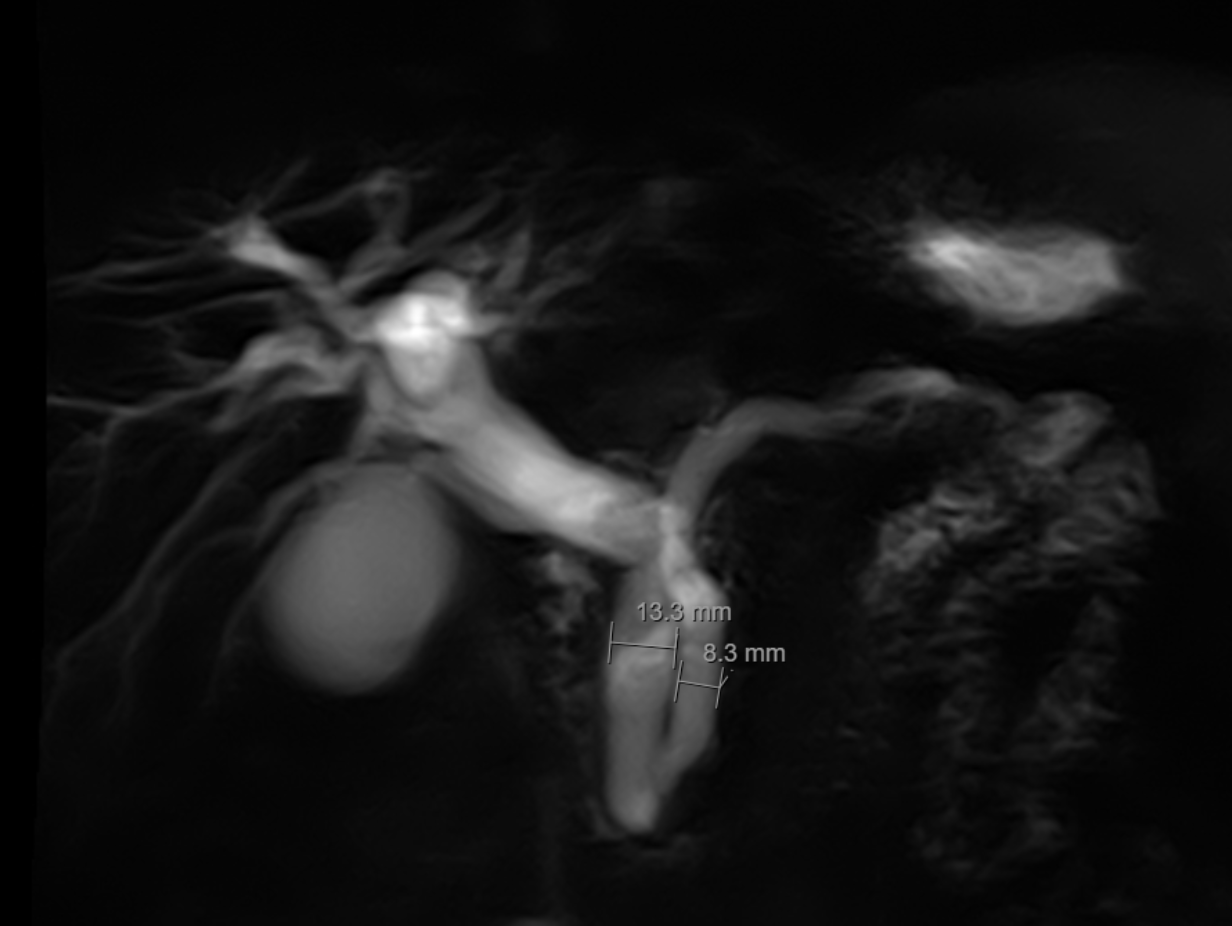
Figure: MRCP: CBD measures 13 mm in width and the main pancreatic duct measures 8 mm in width. With no evidence of an obstructing lesion.
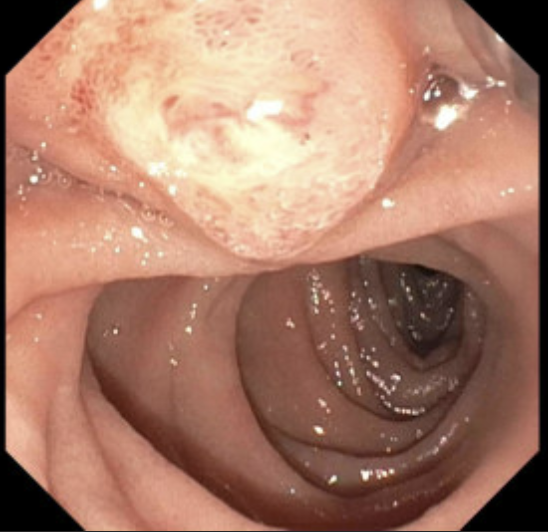
Figure: EGD finding of Type III Choledochocele
Disclosures: Ganesh Ramaprasad indicated no relevant financial relationships. Angela Baquiran indicated no relevant financial relationships. Chetan Pai indicated no relevant financial relationships.
Ganesh Ramaprasad, MD, Angela Baquiran, MD, Chetan Pai, DO. P4476 - Type III Choledochocele Coexisting With Neurofibromatosis 1: An Unusual Case of Silent Biliary Cyst, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.