Abdullah A. Memon, MD1, Michael G. Horton, MD2, Alexis Serrano, DO2 1Northwestern Medicine, Chicago, IL; 2Northwestern Medicine, Palos Heights, IL Introduction: Bile duct injury is a known complication of cholecystectomy, with higher rates in patients undergoing robotic assisted cholecystectomy compared to laparoscopic or open cholecystectomy. We present a case of a patient who underwent robotic cholecystectomy for cholecystitis and was found to have a bile leak requiring ERCP with stent placement and biliary drain placement, subsequently developing peritonitis and hematoma requiring another drain placement.
Case Description/
Methods: A 25-year-old female with no significant past medical history presented with abdominal pain and work up consistent with cholecystitis s/p robotic cholecystectomy. A small amount of bile leak was noted from the cystic plate which was controlled with cautery and Tisseel. She then presented a few days later with fever, nausea, vomiting and abdominal pain with HIDA scan showing small to moderate volume bile leak. She underwent ERCP where deep access was not achieved but cholangiogram showed leak in the right system, and short sphincterotomy was made. Repeat ERCP again demonstrated massive leaking at the common hepatic duct and right intrahepatic system, and a biliary stent was placed. Patient had worsening pain the next day, and MRCP showed increase in abdominal fluid collection, thus percutaneous ductal drain was placed with bilious fluid output. Unfortunately, the patient continued to decline with imaging suggestive of peritonitis and developing hematoma in drain cavity with worsening ascites. IR then placed a second drain with bloody output. The patient was transferred to a tertiary medical center where she underwent exploratory laparotomy with abdominal washout with around 3 liters of fluid drained and irrigated. Two stents were placed in branches of left and right intrahepatic ducts during a third ERCP, as there was concern for transected right main hepatic duct. Percutaneous transhepatic drain was also placed by IR for additional control. Discussion: Bile duct injury is a significant cause of morbidity and mortality, especially when not recognized intraoperatively. Risk factors of bile duct injury include anatomic variance, patient condition, gallbladder pathology and surgeon related factors. Patients typically present with fever, abdominal pain and nausea, and the injury manifests as a biliary obstruction, leak or stricture. Imaging modalities to evaluate include ultrasound, CT, HIDA scan and MRI. Treatment of bile duct injuries depends on the complexity of the injury, from drains to reconstruction of the biliary system.
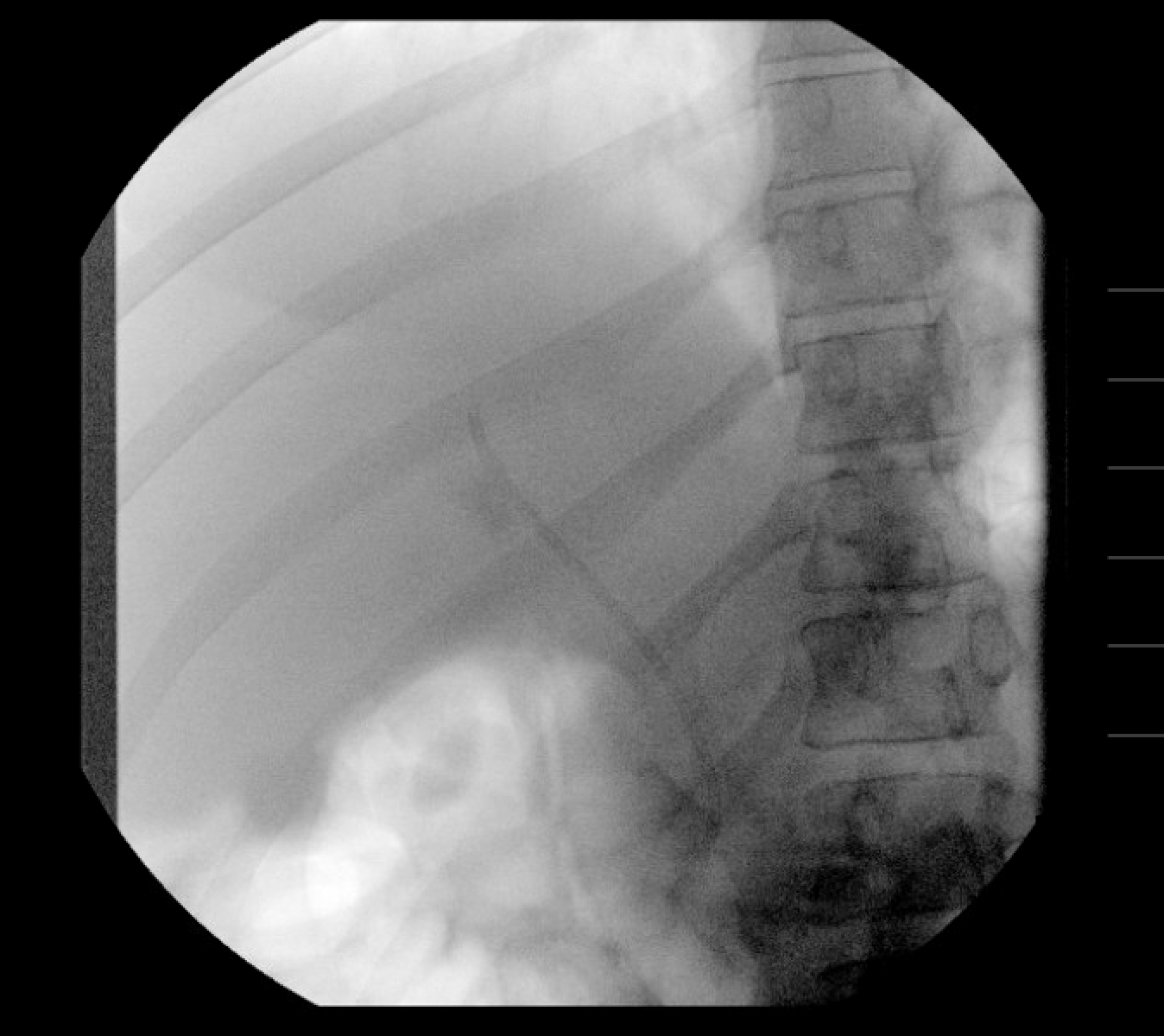
Figure: Cholangiogram during second ERCP showing right intrahepatic system injury.
Figure: Cholangiogram during second ERCP showing placement of a 7 French 9 cm plastic biliary stent.
Disclosures: Abdullah Memon indicated no relevant financial relationships. Michael Horton indicated no relevant financial relationships. Alexis Serrano indicated no relevant financial relationships.
Abdullah A. Memon, MD1, Michael G. Horton, MD2, Alexis Serrano, DO2. P4473 - Complications Related to Bile Duct Injury During Robotic Cholecystectomy: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.