Montefiore St Luke's Cornwall Hospital Newburgh, NY
Anastasiia Babintseva, MD, Veronica Manchanda, MD, Nashwa Ali, MD, Suchith Boodegere Suresh, Montefiore St Luke's Cornwall Hospital, Newburgh, NY Introduction: Raoultella ornithinolytica is a Gram-negative, encapsulated, non-motile bacillus of the Enterobacteriaceae family, previously classified within the Klebsiella genus. Although increasingly recognized as a human pathogen, R. ornithinolytica remains rare and is most often associated with biliary infections, particularly in malignancy. We describe a cirrhotic patient with acute cholecystitis and R. ornithinolytica bacteremia managed via percutaneous transhepatic cholecystostomy (PTC).
Case Description/
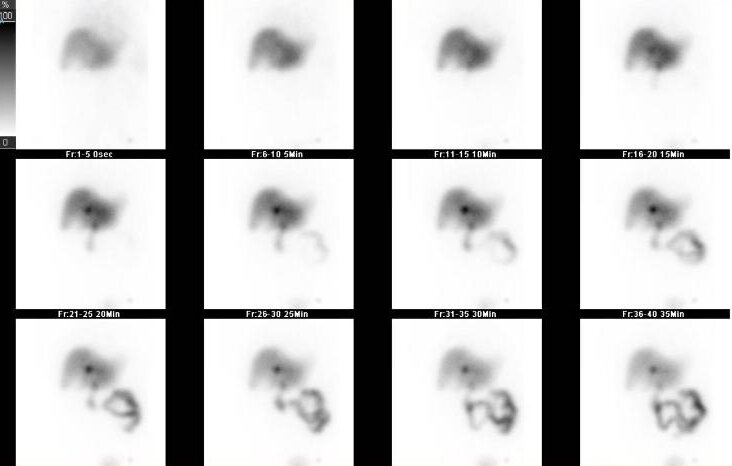
Methods: A 49-year-old male with compensated alcoholic cirrhosis (abstinent 10 years) presented with right upper quadrant (RUQ) pain, nausea, vomiting, fever, and chills. Exam showed RUQ tenderness and a positive Murphy’s sign. Labs revealed lactic acidosis (3.4 mmol/L), cholestatic pattern (AST 64 U/L, ALT 77 U/L, ALP 138 U/L), leukopenia (WBC 2.8 × 10³/µL), thrombocytopenia (81 × 10³/µL), and anemia (Hb 11.2 g/dL). US showed gallbladder distention with sludge and hepatomegaly. IV fluids, analgesia, and broad-spectrum antibiotics were started. Blood cultures grew R. ornithinolytica sensitive to third-generation cephalosporins; antibiotics were narrowed to ceftriaxone and metronidazole. By day 2, platelets declined to 41 × 10³/µL with new hematuria and persistent RUQ pain. CT showed cirrhosis, splenomegaly, and unchanged gallbladder findings. HIDA confirmed cystic duct obstruction (Figure 1). Surgery deferred cholecystectomy due to thrombocytopenia; US-guided PTC was placed. The patient improved and was discharged on day 7 with a cholecystostomy tube and 7-day oral cefuroxime and metronidazole. Four weeks later, he re-presented with RUQ discomfort and change in catheter output to orange-brown, concerning for acute-on-chronic cholecystitis. IV antibiotics were restarted. Imaging showed no obstruction; blood cultures were sterile. The tube was removed per surgical advice. He was counseled on chronic cytopenias and declined HIV testing. He improved and was discharged. Discussion: This case highlights R. ornithinolytica’s ability to cause severe cholecystitis with bacteremia. Cirrhosis and thrombocytopenia complicated surgical management, necessitating percutaneous intervention. As an emerging pathogen, it should not be dismissed as a contaminant. Its potential for community-acquired infection and drug resistance poses a serious sepsis risk. To our knowledge, this is one of few reported cases successfully managed with cholecystostomy. Awareness of its pathogenicity is essential in high-risk patients.
Figure: Figure 1. HIDA scan images (0–35 minutes) showing normal hepatic uptake and biliary excretion with persistent non-visualization of the gallbladder, consistent with cystic duct obstruction and acute cholecystitis.
Disclosures: Anastasiia Babintseva indicated no relevant financial relationships. Veronica Manchanda indicated no relevant financial relationships. Nashwa Ali indicated no relevant financial relationships. Suchith Boodegere Suresh indicated no relevant financial relationships.
Anastasiia Babintseva, MD, Veronica Manchanda, MD, Nashwa Ali, MD, Suchith Boodegere Suresh, . P4460 - An Unusual Culprit in Cholecystitis: <i>R. Ornithinolytica</i> In a Cirrhotic Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.