Fnu Soxi, MD1, Fnu Warsha, MD2, Fnu Avinash, MD3, Fnu Anum, MD4, Fnu Vishaka, 5 1Jersey City Medical Center, Jersey City, NJ; 2Norton Healthcare, Norton, VA; 3University of California Irvine Health, Anaheim, CA; 4Mayo Clinic, Jacksonviile, FL; 5Jinnah Sindh Medical University, Karachi, Sindh, Pakistan Introduction: Hepatic hydrothorax (HH) is the accumulation of transudative pleural effusion in patients with chronic liver disease and portal hypertension, excluding cardiac, pulmonary, and renal causes. It is a less common complication of portal hypertension, affecting 5% to 15% of such patients.
Case Description/
Methods: A 44-year-old female with a history of hypertension, hypothyroidism, and decompensated cirrhosis due to PSC presented with worsening dyspnea, chest heaviness, and bilateral lower extremity edema over three days. She had a history of hepatocellular carcinoma (HCC) in remission and recurrent right-sided pleural effusions due to HH, necessitating multiple thoracenteses. Despite prior hospitalizations for acute hypoxic respiratory failure and treatment with antibiotics, albumin, and oxygen therapy, she continued experiencing respiratory symptoms and volume overload, partly attributed to intravenous fluid administration.
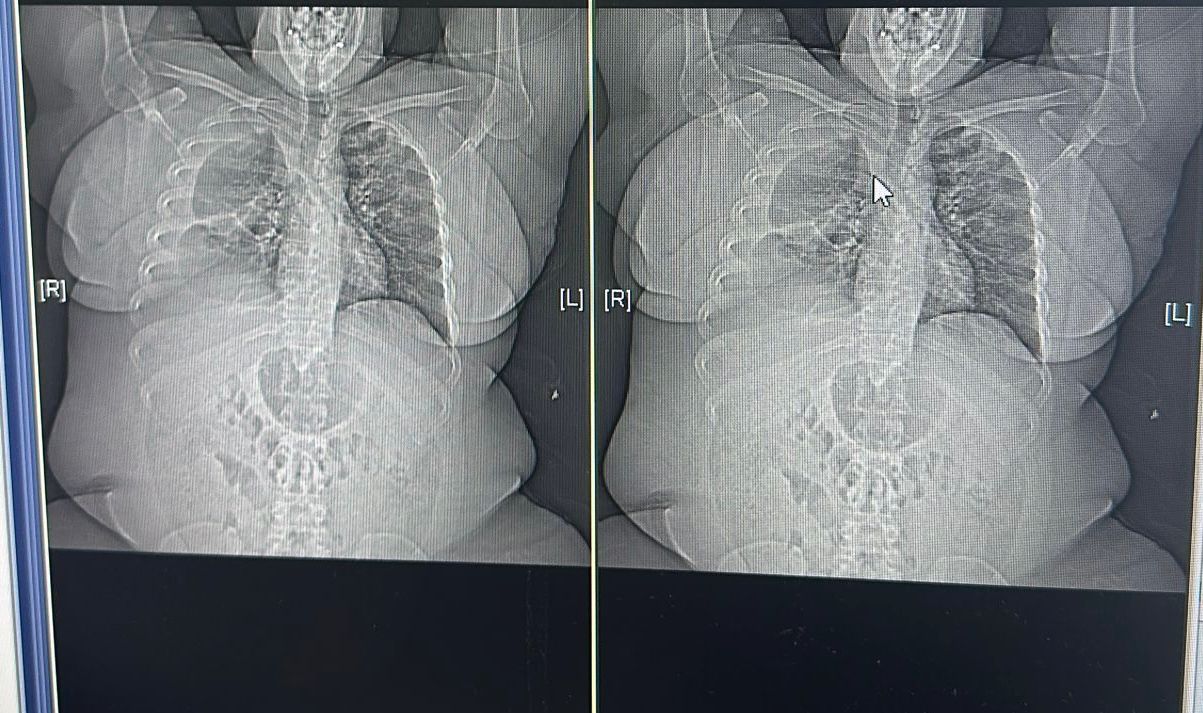
On physical examination, signs of fluid overload were evident, including bilateral pitting edema and right lower chest dullness on percussion, indicative of HH. Laboratory tests showed creatinine 1.7 mg/dL, hypoalbuminemia (2.1 g/dL), and elevated bilirubin (4.2 mg/dL), consistent with liver dysfunction and cholestasis. Imaging showed significant right-sided pleural effusion and diaphragmatic depression, with no HCC recurrence. Her condition highlighted the severe complications of PSC, particularly HH, and the potential progression to hepatorenal syndrome. Discussion: Recurrent HH in PSC indicates severe hepatic decompensation and poor prognosis, requiring close attention. Symptoms can range from asymptomatic to life-threatening respiratory failure. Accurate diagnosis through pleural fluid analysis and timely intervention are critical for successful HH management.
HH arises from the translocation of more than 500 mL of ascitic fluid into the pleural cavity through diaphragmatic defects, exacerbated by increased intra-abdominal pressure and hypoalbuminemia. Its management requires a multidisciplinary approach involving sodium restriction, diuretics, and therapeutic paracentesis. Refractory cases may benefit from transjugular intrahepatic portosystemic shunt. First-line treatment includes salt restriction and diuretics. However, if diuretics fail or cause renal complications, repeated thoracenteses may relieve respiratory symptoms. Frequent procedures, however, carry risks such as infections and protein loss. Liver transplantation is the definitive treatment for refractory HH.
Figure: Primary Sclerosing Cholangitis (PSC) Leading to Recurrent Hepatic Hydrothorax
Disclosures: Fnu Soxi indicated no relevant financial relationships. Fnu Warsha indicated no relevant financial relationships. Fnu Avinash indicated no relevant financial relationships. Fnu Anum indicated no relevant financial relationships. Fnu Vishaka indicated no relevant financial relationships.
Fnu Soxi, MD1, Fnu Warsha, MD2, Fnu Avinash, MD3, Fnu Anum, MD4, Fnu Vishaka, 5. P4446 - A Case of Severe Primary Sclerosing Cholangitis (PSC) Leading to Recurrent Hepatic Hydrothorax, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.