Lake Erie College of Osteopathic Medicine Erie, PA
Martin Ankamah, MBA1, Robert S. Aaron, MD2 1Lake Erie College of Osteopathic Medicine, Erie, PA; 2Allied Digestive Health (Middlesex Monmouth Gastroenterology), Freehold, NJ Introduction: Lemmel syndrome is a rare, pancreaticoduodenal condition that can be challenging to diagnose since other gastrointestinal diseases can have similar clinical presentations. It is characterized by a periampullary duodenal diverticulum that causes compression and dilation of the common bile duct (CBD). Patients may present with elevated bilirubin and liver enzymes, obstructive jaundice, or right upper quadrant pain. Other risk factors are diverticulitis, a history of gallstones, and a patient’s age. Treatments vary based on the severity of the symptoms and can include IV antibiotics, nasogastric decompression, or surgery. The objective of this clinical vignette is to add to current knowledge by underscoring the breadth of clinical presentations of Lemmel syndrome.
Case Description/
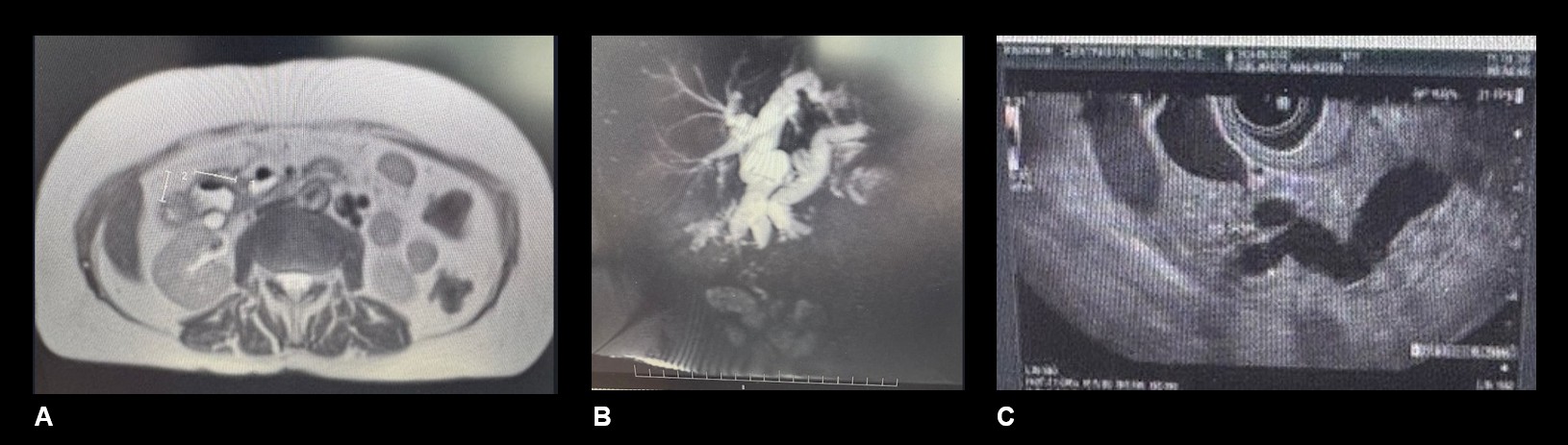
Methods: An 81-year-old woman with a past medical history significant for myasthenia gravis, colon polyps, and Barrett's esophagus was admitted to the hospital for evaluation of right upper quadrant pain. Liver function testing was normal. CT scan of the abdomen and pelvis with contrast demonstrated dilation of the CBD to approximately 1.5 cm and dilation of the pancreatic duct. An MRI/MRCP was performed, which demonstrated findings suggestive of Lemmel syndrome with a prominent periampullary diverticulum causing compression of the CBD and significant dilation of the intrahepatics and CBD to 15 mm. The pancreas was also noted to be atrophic with diffuse pancreatic ductal dilation. A subsequent endoscopic ultrasound was performed, which demonstrated a dilated pancreatic duct at 7 mm, a dilated CBD at 13 mm, and a diverticulum in the second portion of the duodenum. The pancreas appeared normal. Discussion: This clinical vignette highlights the need for continued high, clinical suspicion from physicians when patients present with right upper quadrant pain or jaundice. One consideration for physicians is to include Lemmel syndrome as a potential differential diagnosis that needs to be considered for patients with a past medical history of diverticulitis and right upper quadrant pain or jaundice. As the knowledge around this disease continues to evolve, clinicians will likely become able to identify potential risk factors that strongly indicate a basis for evaluation of asymptomatic patients who are at risk.
Figure: A. duodenal diverticulum, MRI abdomen B. cholangiogram, MRCP C. ductal system, EUS
Disclosures: Martin Ankamah indicated no relevant financial relationships. Robert Aaron indicated no relevant financial relationships.
Martin Ankamah, MBA1, Robert S. Aaron, MD2. P4443 - Lemmel Syndrome: A Rare Cause of Right Upper Quadrant Pain and Chronic Pancreatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.