KASTURBA MEDICAL COLLEGE,MANIPAL Manipal, Karnataka, India
Anmol Malhotra, MBBS, MD, Shiran Shetty, MBBS, MD, DM KASTURBA MEDICAL COLLEGE,MANIPAL, Manipal, Karnataka, India Introduction: Lemmel syndrome is a rare cause of obstructive jaundice due to extrinsic compression of the common bile duct by a periampullary duodenal diverticulum, occurring in the absence of stones or malignancy. Although duodenal diverticula are common, only a small fraction are periampullary and symptomatic. Diagnosis is often incidental, as clinical signs are nonspecific and frequently mimic pancreatic or biliary tumors. MRCP is useful for non-invasive evaluation, while ERCP remains the gold standard for both diagnosis and treatment. Management is individualized due to its rarity and variable presentation. We present a rare case of Lemmel syndrome presenting with recurrent cholangitis and intermittent jaundice, emphasizing the need for high clinical suspicion in similar scenarios.
Case Description/
Methods: A 50-year-old male with no prior comorbidities presented with intermittent, colicky epigastric pain for one year, aggravated postprandially and occasionally associated with fever. Initial evaluation showed cholestatic injury -transaminitis (ALT 464 U/L, AST 664 U/L), elevated ALP (270U/L), total bilirubin 1.8 mg/dL, and lipase 137 U/L. Abdominal ultrasound was unremarkable. CECT revealed a distal extrinsic compression with evidence of a periampullary diverticulum. MRCP confirmed a periampullary duodenal diverticulum compressing the CBD, consistent with Lemmel syndrome.
Initial ERCP failed to achieve biliary stenting; only papillotomy was performed. The patient showed temporary clinical improvement. He later developed scleral icterus and recurrent cholangitis, with worsening liver function tests (peak bilirubin 5.7 mg/dL). Repeat ERCP revealed a dilated CBD, tortuous cystic duct with low insertion. Selective cannulation was achieved, and a biliary stent was successfully placed. Post-procedure, the patient had marked clinical and biochemical improvement and remained asymptomatic on follow-up.
Discussion: This case illustrates Lemmel syndrome as a rare cause of recurrent cholangitis and highlights repeat ERCP as a viable non-surgical treatment option when performed by experienced endoscopists familiar with altered periampullary anatomy.It is a rare cause of obstructive jaundice due to periampullary duodenal diverticulum compressing the CBD. It should be considered when imaging shows no stones or tumors. Diagnosis requires high suspicion and advanced imaging. ERCP offers both diagnosis and treatment . Increased awareness is key to avoiding misdiagnosis and unnecessary surgery.
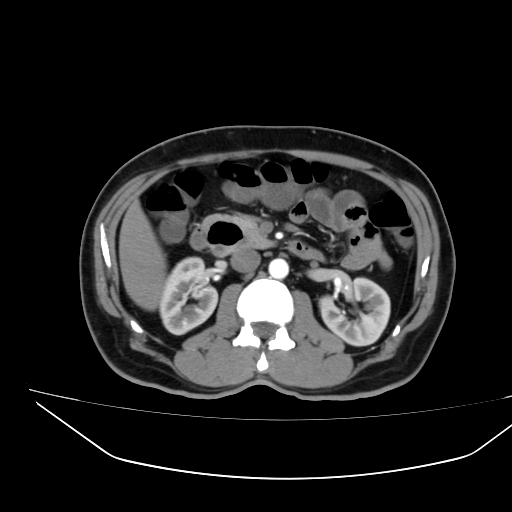
Figure: CECT abdomen showing evidence of periampullary diverticulum
Figure: ERCP showing periampullary diverticulum for which Biliary cannulation and stenting was done.
Disclosures: Anmol Malhotra indicated no relevant financial relationships. Shiran Shetty indicated no relevant financial relationships.
Anmol Malhotra, MBBS, MD, Shiran Shetty, MBBS, MD, DM. P4434 - The Phantom Obstruction: Lemmel Syndrome Causing Recurrent Cholangitis Without Stones, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.