John Nahas, MD1, Mahesh Tummala, DO1, Livasky Concepcion Perez, MD2 1HCA Healthcare, Aventura, FL; 2HCA Florida Healthcare, Aventura, FL Introduction: Acute liver failure (ALF) is defined by the three criteria of 1. transaminitis, jaundice, and RUQ pain 2. Encephalopathy and 3. INR > 1.5. While rare, ALF occurs in approximately 1% of cases of acute Hepatitis B viral infection. Initiation of antiviral therapy with tenofovir or entecavir monotherapy as well as evaluation for liver transplant is the standard of care.
Case Description/
Methods: A 47 year old woman with no PMH presented for one week history of worsening malaise, nausea, vomiting, and worsening jaundice. Labs showed the patient was in ALF with AST of 2124 u/L, ALT 3114 u/L, Alkaline phosphatase of 361 u/L, hyperammonemia of 63 mcmol/l, and INR of 6.6. The patient has no known chronic hepatic disease. Patient was not encephalopathic. She denied alcohol consumption, IV drug use, or acetaminophen use. She did report daily use of 1-2 energy drinks. She also reported recent diagnosis of Hepatitis B with her physician after finding a new sexual partner several months prior to hospital admission. Gastroenterology was consulted and recommended transfer to transplant facility. Vitamin K, lactulose, Tenofovir, and NAC were initiated. Active HBV confirmed on viral hepatitis panel. This presentation was suspicious for ALF, with acute HBV infection and possible component of DILI.
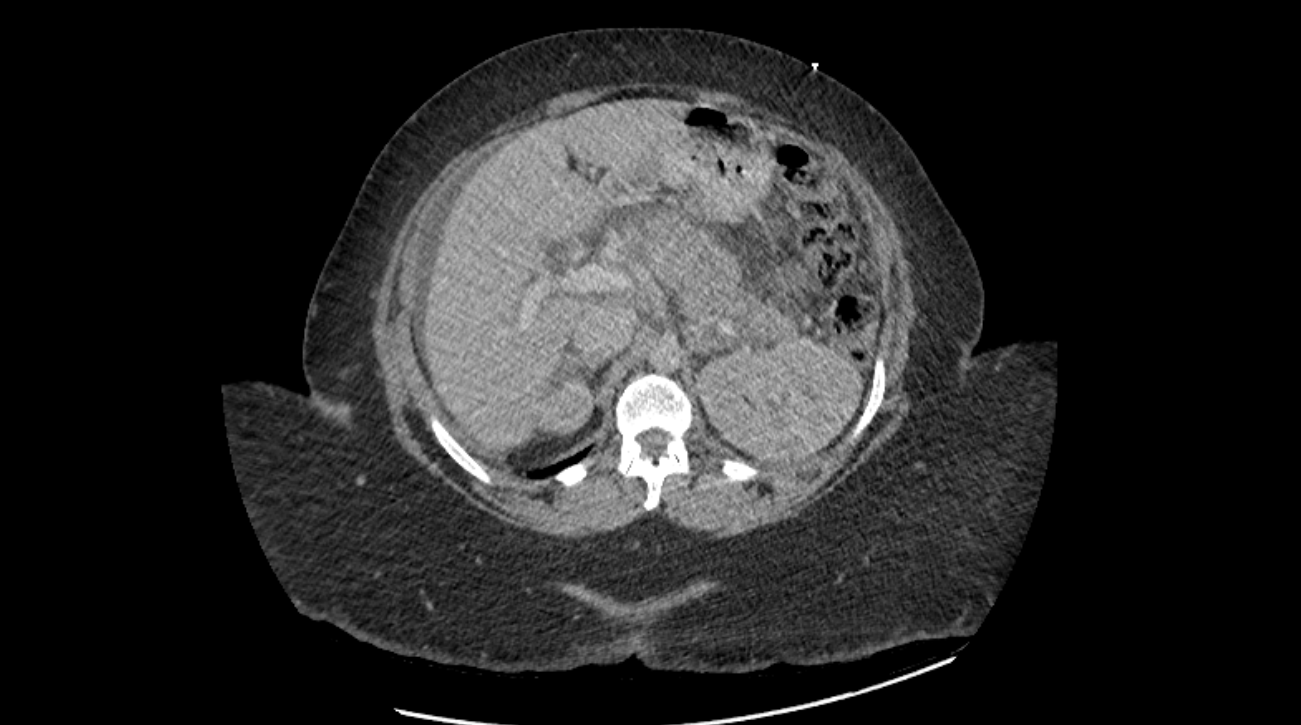
During the patient’s stay in the ICU, she reported a new onset severe abdominal pain, radiating to the back. CT Abdomen/Pelvis showed inflamed pancreas with infiltration of the surrounding fat consistent with pancreatitis. RUQ US negative for gallstone. This clinical picture was concerning for acute pancreatitis second to Tenofovir use. Further workup was halted due to acceptance to transplant institute. Discussion: NRTI-induced pancreatitis has been described in HIV patient’s receiving combination NRTI regimens including didanosine + tenofovir and bictegravir, emtricitabine, and tenofovir. The literature has clearly demonstrated evidence of mitochondrial toxicity as the major cause of NRTI-induced myopathy, neuropathy, lipoatrophy, and lactic acidosis.. Some evidence suggests mitochondrial toxicity is also implicated in the pathway causing pancreatitis as well. In summary, considering the timing of Tenofovir induction and the onset of symptoms, worsening leukocytosis, and radiological findings, we witness a case of likely tenofovir induced pancreatitis. Common, alternative etiologies were ruled out. We see here an interesting presentation of NRTI-induced pancreatitis in the setting of ALF.
Figure: Massively inflamed body and tail of pancreas on CT with infiltration of the surrounding fat
Disclosures: John Nahas indicated no relevant financial relationships. Mahesh Tummala indicated no relevant financial relationships. Livasky Concepcion Perez indicated no relevant financial relationships.
John Nahas, MD1, Mahesh Tummala, DO1, Livasky Concepcion Perez, MD2. P4432 - NRTI-Induced Pancreatitis Second to Viral-Induced Acute Liver Failure, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.