Rachel Dennis, DO1, Jessica Corder, MD2, Allison Bush, MD3, Matthew A.. Wagner, MD4 1Naval Medical Center Portsmouth, Portsmouth, VA; 2United States Navy, Sasebo, Nagasaki, Japan; 3Uniformed Services University of the Health Sciences, Portsmouth, VA; 4United States Navy, Yokosuka, Kanagawa, Japan Introduction: Meckel’s diverticula is a congenital anomaly of the gastrointestinal tract and can predispose patients to complications such as bleeding, obstruction, inflammation or perforation. Obstruction, when it occurs, is typically caused by the fibrous remnants attaching the diverticulum to the umbilicus.2 In the following case, we discuss a rare complication with a mesodiverticular adhesion from the Meckel’s diverticulum to adjacent mesentery leading to a small bowel obstruction.
Case Description/
Methods: A 23-year-old male with no prior medical history, presented to the emergency department with 2 days of worsening abdominal pain. The patient woke up with nausea without emesis the day before with epigastric pain that moved centrally throughout the day. He endorsed one episode of non-bloody loose stool when the pain started. However, shortly afterward experienced obstipation. He denied any recent sick contacts, unusual food exposures, new ingestions or long-term NSAID use, though he endorsed trying NSAIDs without relief of pain.
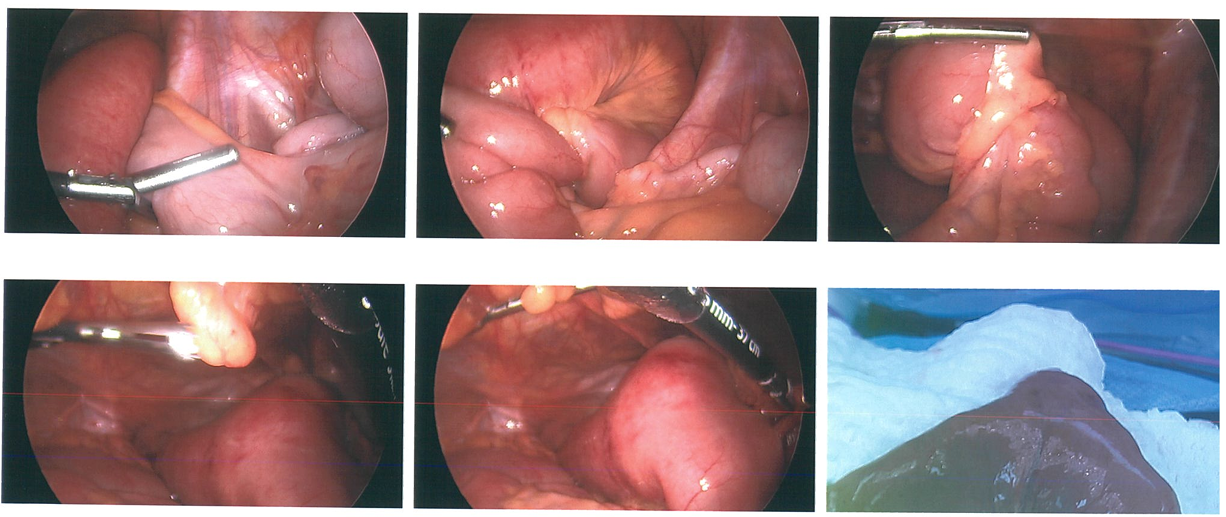
Upon presentation to the emergency department, vital signs were within normal limits. His abdomen was mildly distended with rebound tenderness and guarding primarily in the lower quadrants, concerning for peritonitis. White blood cell count was elevated at 11.3 with neutrophil predominance. Hemoglobin was elevated at 16.8 and albumin elevated at 5.3. A stat computed tomography of the abdomen revealed a distal small bowel obstruction with transition point at an inflamed appearing loop of distal small bowel. The patient was emergently taken back to the operating room where he was found to have an adhesive band extending from the tip of a Meckel’s diverticulum to the adjacent small bowel mesentery. It had a clear transition point between dilated bowel proximally and decompressed bowel distally. The diverticulum was 2-3cm in diameter and a small bowel resection was performed. Discussion: Meckel’s diverticulum can present with a variety of complications, including obstruction, intussusception, inflammation, diverticulitis, and perforation hemorrhage, neoplasm or fistula.3 However, the majority of these obstructions typically occur from volvulus around fibrous bands adherent to the umbilicus. Inflammatory lesions, particularly between the diverticulum and the mesentery, are much less common but can lead to loop formations causing incarceration of the distal ileum.
Figure: Adhesive band extending from Meckel's diverticulum to the adjacent small bowel mesentery.
Disclosures: Rachel Dennis indicated no relevant financial relationships. Jessica Corder indicated no relevant financial relationships. Allison Bush indicated no relevant financial relationships. Matthew Wagner indicated no relevant financial relationships.
Rachel Dennis, DO1, Jessica Corder, MD2, Allison Bush, MD3, Matthew A.. Wagner, MD4. P1999 - Meckel's Diverticulum With Mesodiverticular Adhesions Leading to Small Bowel Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")