Prisma Health Greenville Memorial Hospital Greenville, SC
Aaron Rampersad, DO, Jay Alden, DO, Graziella Rangel Paniz, MD Prisma Health Greenville Memorial Hospital, Greenville, SC Introduction: Distant metastasis of lung cancer frequently involves the bone, brain, liver, and adrenal glands. However, lung cancer metastasizing to the intraluminal small bowel is very rare and often remains undetected until late in the disease course. We present a case of metastatic lung adenocarcinoma to the terminal ileum diagnosed by colonoscopy with biopsy and immunohistochemical staining.
Case Description/
Methods: A 56-year-old Caucasian female with a history of recurrent non-small cell lung adenocarcinoma metastatic to cervical lymph nodes, upper mediastinal lymph nodes, and right neck vasculature, previously treated with chemoradiation and complicated by tumor thrombosis managed on Eliquis, cervical cancer, severe chronic obstructive pulmonary disease, and nicotine use disorder presented with melena for one week. Computerized tomography of the abdomen and pelvis with angiography revealed a long-segment, mass-like thickening of the terminal ileum with adjacent necrotic mesenteric adenopathy measuring 6.7 cm, suspicious for malignancy but without active extravasation. Gastroenterology was consulted, and the patient underwent esophagogastroduodenoscopy, which was unremarkable, followed by colonoscopy with ileoscopy. This revealed a fungating, circumferential, partially obstructing mass with active oozing in the terminal ileum. Pathology showed malignant cells with increased nuclear to cytoplasmic ratio, irregular clear contours, and nuclear hyperchromasia. Immunohistochemical staining revealed positive thyroid transcription factor-1, cytokeratin 7, and focal positivity for Napsin A, while negative for CDX-2 and cytokeratin 20. This immunoprofile confirmed metastatic pulmonary adenocarcinoma to the terminal ileum, excluding a gastrointestinal primary. Given the advanced disease, the patient was transitioned to comfort care and discharged home with hospice services. Discussion: Distant metastasis of non-small cell lung cancer to the intraluminal small bowel is exceedingly rare. It is essential to consider small bowel metastasis from lung cancer in the differential diagnosis for patients with non-specific gastrointestinal symptoms and suggestive imaging findings. Typically, pulmonary adenocarcinoma metastases retain immunoreactivity to markers such as TTF-1 and CK7, facilitating accurate identification by pathology. Prognosis in cases of small bowel metastasis from lung cancer is poor, often with survival measured in weeks to a few months given the advanced presentation and limited therapeutic options.
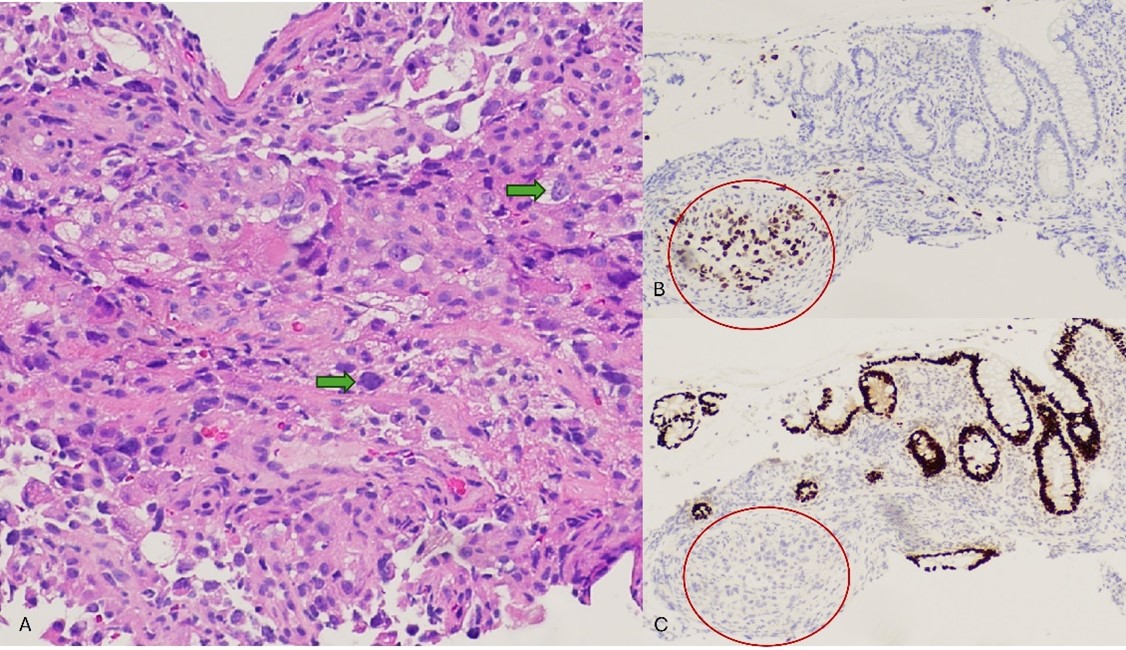
Figure: The biopsy showed small bowel mucosa involved by malignant cells with increased nuclear to cytoplasmic ratio, irregular clear contours, and nuclear hyperchromasia (Figure A, green arrows). Immunohistochemical stains were performed and revealed the malignant cells to be positive for TTF-1 (Figure B, right circled area), CK7, and focally for Napsin A. Tumor cells were negative for CDX-2 (Figure C, red circled area) and CK20, which highlighted the background benign intestinal epithelium. This immunoprofile is consistent with metastatic pulmonary adenocarcinoma and militates against a gastrointestinal primary.
Figure: Figure C and D: Colonoscopy with ileoscopy showing fungating, circumferential, partially obstructing mass with active oozing in the terminal ileum.
Disclosures: Aaron Rampersad indicated no relevant financial relationships. Jay Alden indicated no relevant financial relationships. Graziella Rangel Paniz indicated no relevant financial relationships.
Aaron Rampersad, DO, Jay Alden, DO, Graziella Rangel Paniz, MD. P1996 - Silent Invader: Unexpected Terminal Ileum Metastasis From Lung Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.