Mohamed K.. Osman, MD, MPH1, Stuti Manandhar, MD1, Alvaro Genao, MD2, Joan A.. Culpepper-Morgan, MD, FACG2 1NYC Health + Hospitals/Harlem, New York, NY; 2NYC Health + Hospitals, New York, NY Introduction: Small bowel cancers are rare with incidence of 2.6/100,000, with higher incidence of 4.6 in Blacks. Adenocarcinomas are the second most common type of small bowel cancer after carcinoids. Most arise in the duodenum, followed by jejunum and ileum. We report a case of jejunal small bowel adenocarcinoma in a young African man.
Case Description/
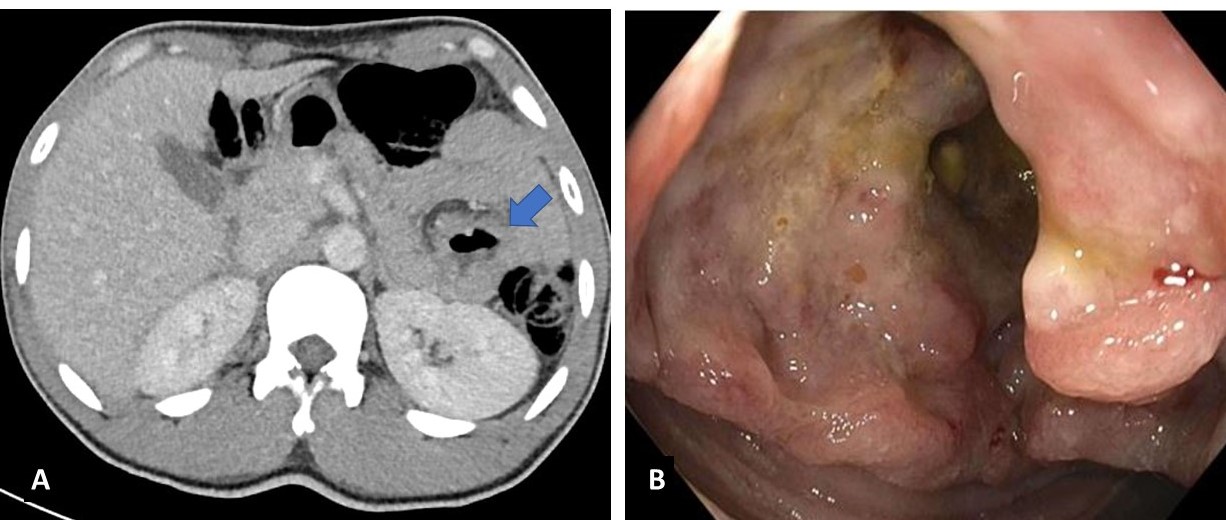
Methods: A 30-year-old Senegalese man presented with 4-years of RUQ abdominal pain, 2-years of dark stools, now worsening over 4 months. He denied tobacco and alcohol use. He had iron deficiency anemia with Hb of 5.5 g/dl, hematocrit 22.7%, MCV 63.9 Fl, ferritin 3 ng/ml, iron 10 ug/dl, TIBC 382 ug/dl, and iron saturation 3%. BUN was 6 mg/dl, and creatinine 0.6 mg/dl. Albumin was 4 g/dl, total protein 7.3 g/dl, total bilirubin 0.2 mg/dl, direct bilirubin < 0.2 g/dl, ALK 49 U/l, ALT 7 U/l, and AST 27 U/l. CT showed a 2.8 cm mild focal dilatation with thickening/nodularity in a small bowel loop at the left upper abdomen with mesenteric adenopathy. Push enteroscopy showed a 5 cm fungating ulcerated circumferential non-obstructing jejunal mass (fig). Biopsy revealed moderately differentiated adenocarcinoma. Gastric biopsy showed chronic active gastritis loaded with H. pylori. Colonoscopy was normal. He received 2 units of pRBCs, iron infusions, and standard triple therapy. PET-CT scan showed a hypermetabolic jejunal mass and nonspecific axillo-inguinal lymphadenopathy. Hb improved to 9.8 g/dl. CEA, CA19-9, and Ca 125 were normal. The patient initially declined surgery. But over 3 months developed fatigue, worsened anemia (Hb 3.4 g/dl), and lost 16 lbs. Repeat PET CT scan was unchanged except for small hypermetabolic ascites. He underwent successful robotic mass resection and was discharged with appropriate follow-up. Discussion: Besides the presentation of a rare tumor, our patient’s young age of 30 is also unusual. These tumors usually present in the 7th or 8th decade. Small intestinal tumors have been increasing in African Americans over the last decade. It is unclear if this applies to recent African immigrants. Celiac disease, and inherited GI malignancy syndromes (Lynch syndrome, Peutz-Jeghers syndrome, familial adenomatous polyposis) are associated with small bowel adenocarcinoma. Our patient had no IBD history. There is no known association between H.pylori infection and small bowel cancer. Prognosis is poor with a median survival of 13 months, with better survival seen in patients younger than 60, early grade, early stage, and jejunal location.
Figure: A. CT scan showing a thickened loop of jejunum (arrow) B. Endoscopy showing an ulcerated non-obstructing jejunal mass
Disclosures: Mohamed Osman indicated no relevant financial relationships. Stuti Manandhar indicated no relevant financial relationships. Alvaro Genao indicated no relevant financial relationships. Joan Culpepper-Morgan indicated no relevant financial relationships.
Mohamed K.. Osman, MD, MPH1, Stuti Manandhar, MD1, Alvaro Genao, MD2, Joan A.. Culpepper-Morgan, MD, FACG2. P1986 - A Case of Jejunal Adenocarcinoma in a 30-year-old Man, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.