Penn State Health Milton S. Hershey Medical Center Hershey, PA
Theja V. Channapragada, DO, MBA, MS1, Anirudh Damughatla, DO1, Justin Canakis, DO1, Ahmed Abdulhamid, MD1, John Levenick, MD2, Hadie Razjouyan, MD1 1Penn State Health Milton S. Hershey Medical Center, Hershey, PA; 2Penn State College of Medicine, Hershey, PA Introduction: Duodenal strictures are a rare complication of refractory celiac disease (RCD). While most improve with a strict gluten-free diet (GFD), a subset progresses to high-grade obstruction, requiring advanced intervention. We present a patient with RCD who experienced recurrent duodenal obstructions requiring multiple balloon dilations and ultimately lumen-apposing metal stent (LAMS) placement.
Case Description/
Methods: A 68-year-old woman with celiac disease presented with post-prandial abdominal pain, bloating, and weight loss despite strict adherence to GFD for two years. Her symptoms began in mid-2023 and progressed to gastric outlet obstruction. Initial small bowel enteroscopy (SBE) revealed a benign 2–3 mm duodenal stricture at the third portion of the duodenum (D3) with biopsy showing moderate to severe villous atrophy. Over the next 18 months, she underwent four additional SBEs with balloon dilations up to 15 mm.
In April and May 2025, she was hospitalized twice for recurrent obstructive symptoms. MR enterography showed severe distention with a discrete stricture at mid-D3. She underwent an SBE, but despite balloon dilation to 16 mm, the stricture remained fixed; a repeat SBE showed persistent stenosis, sharp angulation, and ulceration. Intralesional steroids were deferred. Flow cytometry from initial biopsies revealed atypical intraepithelial lymphocytes (CD2+, CD3+, CD7+, CD5–), raising concern for enteropathy-associated T-cell lymphoma. However, repeat biopsies with flow cytometry sent to an outside institution revealed no definitive evidence of lymphoma. Due to the failure of medical and endoscopic therapy, she underwent LAMS placement across the D3 stricture as a bridging measure. Post-procedure, she reported significant symptomatic relief, resumed solid oral intake, and gained 5–6 pounds within two weeks. A surgical gastrojejunostomy is planned once her nutritional status is optimized. Discussion: Duodenal strictures in celiac disease are rare and may arise from chronic inflammation, ulceration, and enteropathy-associated T-cell lymphoma. Refractory strictures, defined by lack of response despite 12 months of GFD, are often associated with type II RCD and raise lymphoma risk. Our patient followed a strict GFD, avoided NSAIDs, and had a negative malignancy workup. Management begins with GFD and endoscopic balloon dilation, with surgery reserved for refractory cases. In select patients, LAMS placement provides a minimally invasive option when conventional approaches are unsuccessful.
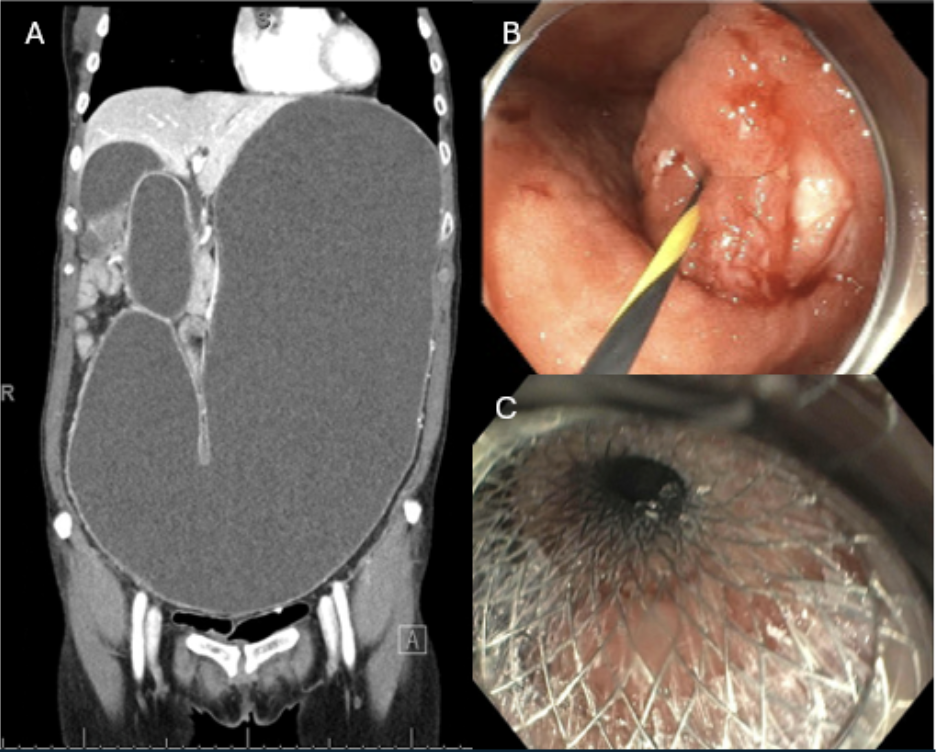
Figure: Figure 1: A: Coronal view of CT A/P w/contrast showing significant gastric outlet obstruction B: Small Bowel Enteroscopy showing fixed 1 mm D3 stricture with evidence of chronic inflammation C: Post-placement of lumen-apposing metal stent across the D3 stricture
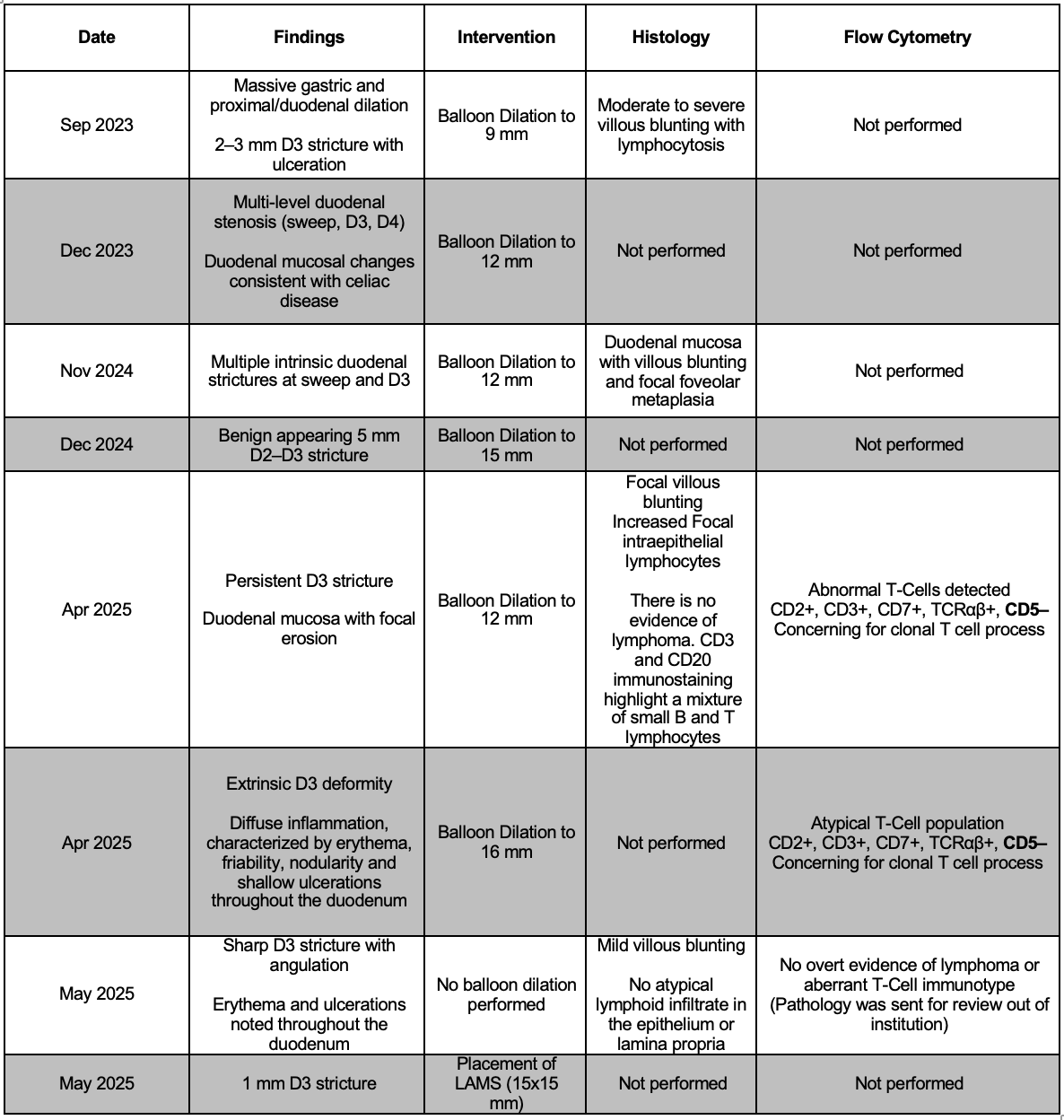
Figure: Table 1: Small Bowel Enteroscopies: Findings, Intervention, Histology, and Flow Cytometry
Disclosures: Theja Channapragada indicated no relevant financial relationships. Anirudh Damughatla indicated no relevant financial relationships. Justin Canakis indicated no relevant financial relationships. Ahmed Abdulhamid indicated no relevant financial relationships. John Levenick indicated no relevant financial relationships. Hadie Razjouyan indicated no relevant financial relationships.
Theja V. Channapragada, DO, MBA, MS1, Anirudh Damughatla, DO1, Justin Canakis, DO1, Ahmed Abdulhamid, MD1, John Levenick, MD2, Hadie Razjouyan, MD1. P1975 - Refractory Celiac Disease-Associated Duodenal Strictures Requiring Lumen-Apposing Metal Stent (LAMS): A Therapeutic Bridge in Obstructive Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")