Texas Tech University Health Sciences Center Lubbock, TX
Zeyad Elharabi, MBBS, MS1, Arman Vaghefi, BS2, Ahmed Shukri, MD1, Aljon Pinili, BS3, Houssam Kharrat, MD4 1Texas Tech University Health Sciences Center, Lubbock, TX; 2Rocky Vista University, Colorado Springs, CO; 3Texas Tech University, Lubbock, TX; 4West Texas Digestive Disease Center, Lubbock, TX Introduction: Aortoenteric fistulas (AEFs) are rare but life-threatening causes of gastrointestinal bleeding, most often involving erosion into the duodenum. We present an unusual case of a graft erosion into the proximal jejunum, leading to upper gastrointestinal bleeding, multi-organ dysfunction, and compartment syndrome.
Case Description/
Methods: A 56-year-old male with a history of hypertension, hyperlipidemia, alcohol use disorder, and extensive vascular disease, including right carotid endarterectomy and aortobifemoral bypass with multiple complications, presented with two days of maroon-colored hematemesis and one day of dark red blood per rectum. He also reported severe right lumbar pain and recurrent falls due to generalized weakness.
The patient underwent aortobifemoral bypass on March 9, 2023. Seventeen days later, he developed right femoral anastomotic dehiscence. Approximately nine months later, he was treated for acute on chronic left limb ischemia due to thrombus in the left aortobifemoral graft limb, which was removed. Another nine months later , he presented with occlusion of the same graft limb, requiring thrombectomy.
On current admission (April 2025), he was hypotensive, tachycardic, and hypoxic with altered mental status. Laboratory findings included leukocytosis (WBC 20.4), anemia (Hb 10.6), and elevated lactate. CT imaging was suggestive of upper GI bleeding and raised suspicion for an aortoenteric fistula. He was intubated for airway protection, and bedside EGD revealed erosion of the aortobifemoral graft into the proximal jejunum.
He underwent emergent exploratory laparotomy, explantation of the graft, jejunal repair, and right axillofemoral-femoral bypass. Postoperatively, he developed left lower extremity ischemia requiring SFA endarterectomy, embolectomy, and four-compartment fasciotomy. Anticoagulation was switched from heparin to argatroban due to suspected failure. Discussion: This case highlights a rare variant of aortoenteric fistula, involving erosion into the jejunum rather than the more commonly affected duodenum. The patient’s surgical history was significant for multiple aortobifemoral graft complications over a two-year span, including right femoral anastomotic dehiscence, recurrent thrombotic occlusion of the left graft limb, and multiple vascular revisions. These repeated interventions likely contributed to the eventual graft-enteric erosion.
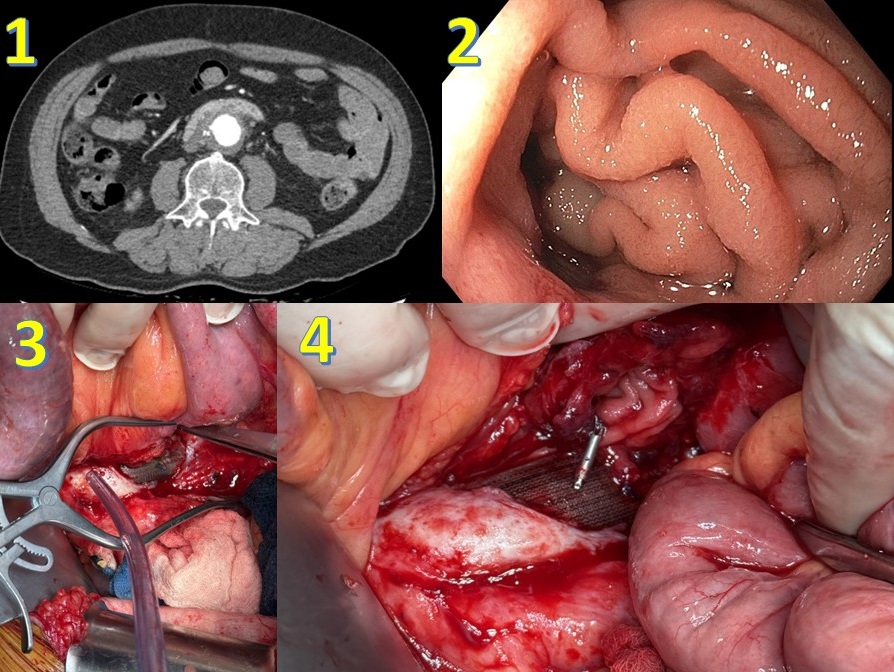
Figure: 1-CT imaging revealed thickened jejunal mucosa with concern for a possible fistulous tract. 2-Upper endoscopy showed a jejunal ulcer with exposed vascular graft material at its base. 3, 4-Surgical exploration confirmed the presence of a large fistulous connection between the graft and the jejunum.
Disclosures: Zeyad Elharabi indicated no relevant financial relationships. Arman Vaghefi indicated no relevant financial relationships. Ahmed Shukri indicated no relevant financial relationships. Aljon Pinili indicated no relevant financial relationships. Houssam Kharrat indicated no relevant financial relationships.
Zeyad Elharabi, MBBS, MS1, Arman Vaghefi, BS2, Ahmed Shukri, MD1, Aljon Pinili, BS3, Houssam Kharrat, MD4. P1970 - Aortoenteric Fistula Beyond the Duodenum: Graft Erosion Into the Proximal Jejunum, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.